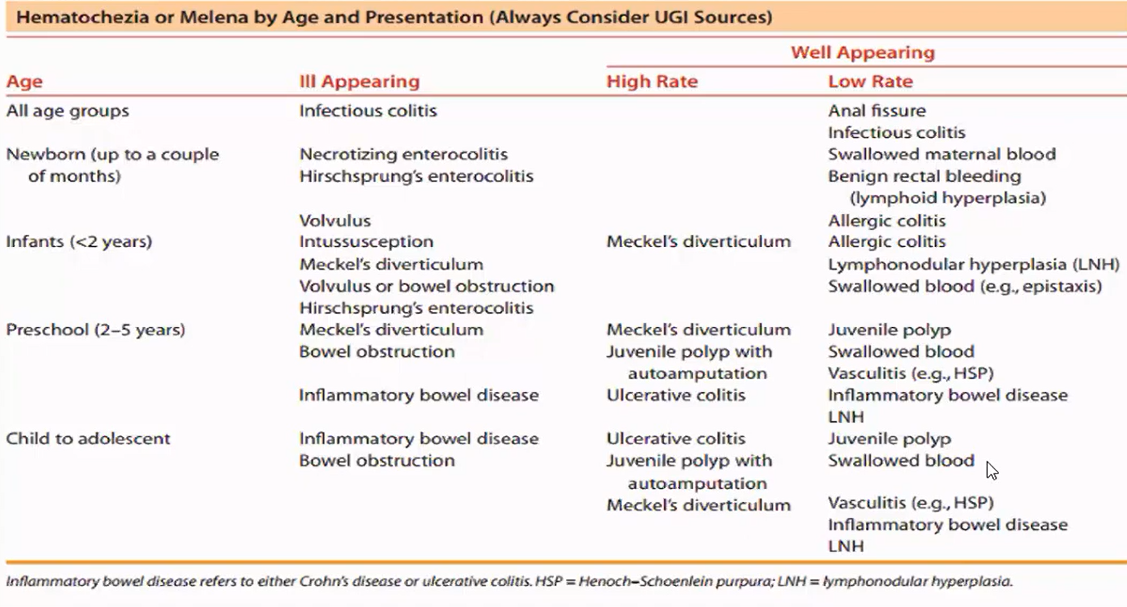
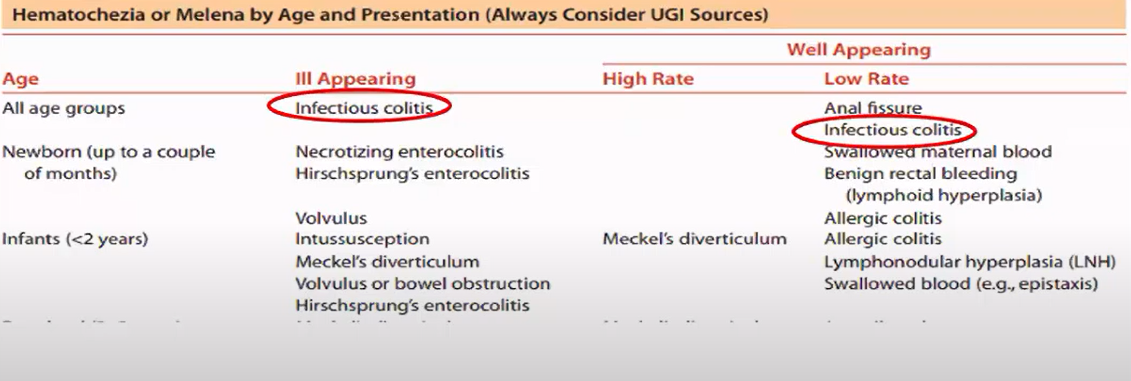
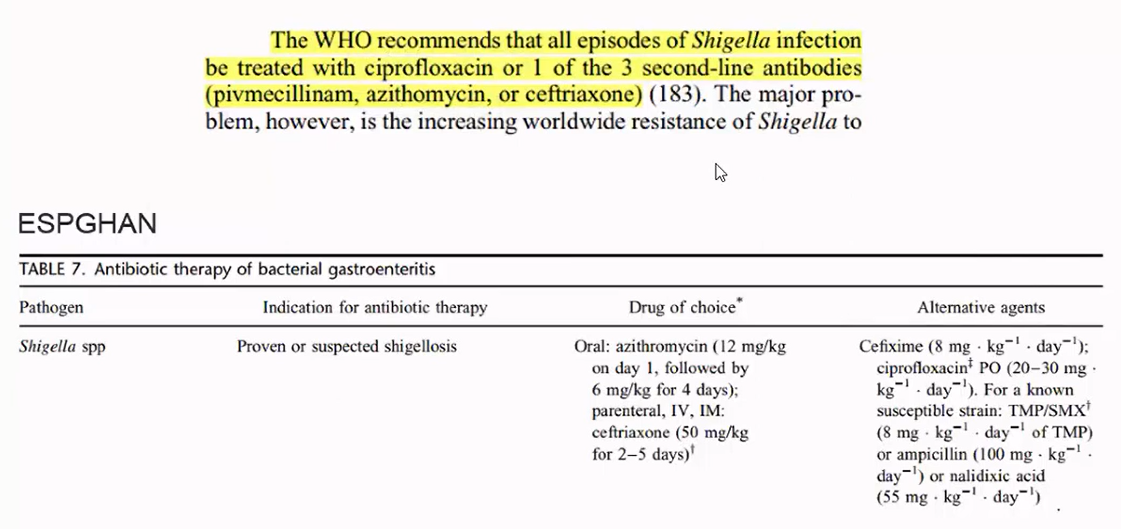
-Nếu nghi ngờ tuổi có khả năng măc Ecoli thì xài Cefa 3 => không dùng Cipro
Azi không nhạy với Shigenlla
-Ở phòng khám: nếu là Lỵ nhẹ thì dùng Cipro uống
-Khi đã vào viện => dùng Cipro truyền; nhưng bé này chỉ là tiêu đàm máu, nghĩ có viêm ruột thôi chứ chưa chắc Shigenlla => Sợ Ecoli nên mới dùng Ceftriaxon ( ngoài ra còn được lợi là chỉ chích 1 lần/ngày là xong)
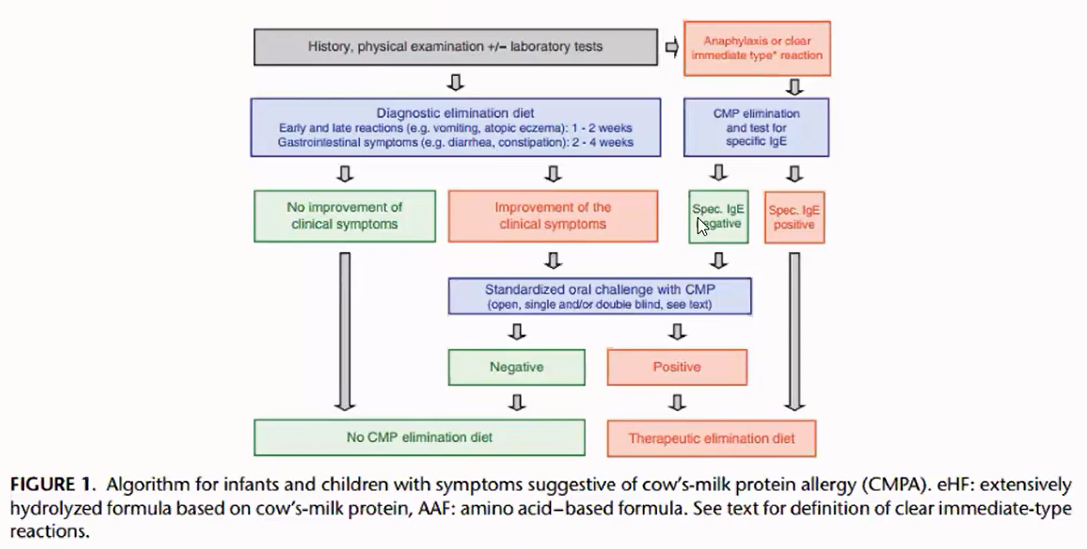
2/ Tiếp cận bé dị ứng đạm sữa bò
*Nếu nghi Dị ứng đạm sữa bò thì phải hỏi kĩ bệnh sử hơn
1/Mẹ ăn chay trường => Thực phẩm chính là gì ? có ăn đậu anh/sản phẩm từ đậu nành không ?
2/ Đây là bé nhẹ cân => Nuôi bằng sữa mẹ hoàn toàn hay không ? lúc sinh ra 1200g, nuôi trong dưỡng nhi có dùng sữa công thức không ? (Yếu tố gợi ý có dùng Similac năng lượng cao, đây là sữa dùng cho trẻ dưỡng nhi để tăng cân) => sữa Similac dùng từ khi nào ?
3/Phân dạng dạng lâm sàng dị ứng sữa bò
-Roclitis => chỉ viêm trực tràng => phân có thể có nhầy máu, không tiêu lỏng
-Roctocolitis => phân lỏng, nhầy, máu
-Enterocolitis => bệnh cảnh: trẻ từ nhỏ tới lớn chưa từng tiếp xúc sữa bò, gần đây mới tiếp xúc, mới => biểu hiện có ói, kèm tiêu lỏng
-Trường hợp dị ứng từ lâu, nên người ta nuôi kết hợp sữa mẹ + sữa công thức hoặc dị ứng luôn cả đậu nành (mẹ ăn đậu nành, qua sữa) => trước đây triệu chứng nhẹ nhẹ, giờ mới nặng lên, thì phân phải đi lỏng từ lâu ( chứ không phải mới xuất hiện 3 ngày như bé này)
4/ Bé này có thiếu máu HC nhỏ, nhược sắc => thuộc trường hợp nào ?
-Mẹ ăn chay trường => thiếu sắt => bé sanh non, sau đó cũng lại được nuôi bằng sữa mẹ thiếu sắt đó => hậu quả TMHCNNS
2023 American Heart Association and American Academy of Pediatrics Focused Update on Neonatal Resuscitation: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Nicole K. Yamada, MD, MS; Edgardo Szyld, MD, MSc, Co-Chair; Marya L. Strand, MD, MS; Emer Finan, MB, MEd; Jessica L. Illuzzi, MD, MS; Beena D. Kamath-Rayne, MD, MPH; Vishal S. Kapadia, MD, MSCS; Susan Niermeyer, MD, MPH; Georg M. Schmölzer, MD, PhD; Amanda Williams, RN, CNS, MSN; Gary M. Weiner, MD; Myra H. Wyckoff, MD; Henry C. Lee, MD, Co-Chair; on behalf of the American Heart Association and American Academy of Pediatrics
DOI: 10.1542/peds.2023-065030
Journal: Pediatrics
Article Type: Special Article
Citation: Yamada NK, Szyld E, Strand ML, et al. 2023 American Heart Association and American Academy of Pediatrics Focused Update on Neonatal Resuscitation: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics. 2023; doi: 10.1542/peds.2023-065030
This is a prepublication version of an article that has undergone peer review and been accepted for publication but is not the final version of record. The journal is providing an early version of this article to expedite access to this information. The American Academy of Pediatrics, the editors, and authors are not responsible for inac- curate information and data described in this version.
2023 American Heart Association and American Academy of Pediatrics Focused Update on Neonatal Resuscitation: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Nicole K. Yamada, MD, MS; Edgardo Szyld, MD, MSc, Co-Chair; Marya L. Strand, MD, MS; Emer Finan, MB, MEd; Jessica L. Illuzzi, MD, MS; Beena D. Kamath-Rayne, MD, MPH; Vishal S. Kapadia, MD, MSCS; Susan Niermeyer, MD, MPH; Georg M. Schmölzer, MD, PhD; Amanda Williams, RN, CNS, MSN; Gary M. Weiner, MD; Myra H. Wyckoff, MD; Henry C. Lee, MD, Co-Chair; on behalf of the American Heart Association and American Academy of Pediatrics
ABSTRACT: This 2023 focused update to the neonatal resuscitation guidelines is based on 4 systematic reviews recently completed under the direction of the International Liaison Committee on Resuscitation Neonatal Life Support Task Force. Systematic reviewers and content experts from this task force performed comprehensive reviews of the scientific literature on umbilical cord management in preterm, late preterm, and term newborn infants, and the optimal devices and interfaces used for administering positive-pressure ventilation during resuscitation of newborn infants. These recommendations provide new guidance on the use of intact umbilical cord milking, device selection for administering positive-pressure ventilation, and an additional primary interface for administering positive-pressure ventilation.
TOP 10 TAKE-HOME MESSAGES FOR NEONATAL RESUSCITATION
For term and late preterm newborn infants ≥34 weeks’ gestation who do not require resuscitation, delayed cord clamping (≥30 seconds) can be beneficial compared with early cord clamping (<30 seconds).
For term and late preterm newborn infants ≥34 weeks’ gestation who do not require resuscitation, intact cord milking is not known to be beneficial compared with delayed cord clamping (≥30 seconds).
For nonvigorous term and late preterm newborn infants (35–42 weeks’ gestation), intact cord milking may be reasonable compared with early cord clamping (<30 seconds).
For preterm newborn infants <34 weeks’ gestation who do not require resuscitation, delaying cord clamping (≥30 seconds) can be beneficial compared with early cord clamping (<30 seconds).
For preterm newborn infants between 28 and 34 weeks’ gestation who do not require resuscitation and in whom
delayed cord clamping cannot be performed, intact cord milking may be reasonable.
For preterm newborn infants <28 weeks’ gestation, intact cord milking is not recommended.
Effective positive-pressure ventilation is the priority in newborn infants who need support after birth.
Using a T-piece resuscitator to deliver positive-pressure ventilation is preferred to the use of a self-inflating bag.
Because both T-piece resuscitators and flow-inflating bags require a compressed gas source to function, a
self-inflating bag should be available as a backup in the event of compressed gas failure when using either of these
Use of a supraglottic airway may be considered as the primary interface to administer positive-
pressure ventilation instead of a face mask for newborn infants delivered at ≥34 0/7 weeks’ gestation.
Abbreviations
AAP
American Academy of Pediatrics
AHA
American Heart Association
COR
class of recommendation
DCC
delayed cord clamping
ILCOR
International Liaison Committee on Resuscitation
LOE
level of evidence
PPV
positive-pressure ventilation
RCT
randomized controlled trial
INTRODUCTION
Scope of the Guidelines
These guidelines are designed for North American health care practitioners caring for newborn infants who are looking for an up-to-date summary for clinical care, and for those who are seeking more in-depth information on these topics in resuscitation science and the gaps in current knowledge. This focused update is based on the systematic reviews of umbilical cord management in term and late preterm infants1 and preterm infants,2 and the devices and interfaces for administering positive-pressure ventilation (PPV).3,4 The findings of those systematic reviews are also reported in the “2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations”5 and the “2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations”6 from the International Liaison Committee on Resuscitation (ILCOR). The guidelines contained in this document serve as an update on these topics from the “2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care”7 and “Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations” from the ILCOR Neonatal Life Support Task Force.8
Organization of the Writing Group
The Neonatal Life Support writing group includes neonatal physicians and nurses with backgrounds in clinical medicine, education, research, and public health. Volunteers with recognized expertise in neonatal resuscitation are nominated by the writing group co-chairs. Writing group members were selected by the American Heart Association (AHA) Emergency
Cardiovascular Care Science Subcommittee and the American Academy of Pediatrics (AAP) Executive Board and then
approved by the AHA Manuscript Oversight Committee.
The AHA and the AAP have rigorous conflict of interest policies and procedures to minimize the risk of bias or improper influence during the development of guidelines. Before their appointment, writing group members disclosed all relevant commercial relationships and other potential (including intellectual) conflicts. Writing group members whose research led to changes in guidelines were required to declare those conflicts during discussions and abstain from voting on those specific recommendations. These procedures are described more fully in “Part 2: Evidence Evaluation and Guidelines Development” of the 2020 guidelines.9
Appendix 1 of this document lists disclosure information and the writing group members’ relevant relationships with
industry.
Methodology and Evidence Review
Updated AHA/AAP guidelines for cardiopulmonary resuscitation and emergency cardiovascular care are developed in concert with ILCOR’s continuous evaluation of new resuscitation science.9 This 2023 focused update is based on 4 systematic reviews completed by the ILCOR Neonatal Life Support Task Force, which reviewed the science on umbilical cord management in preterm, late preterm, and term newborn infants1,2 and on devices and interfaces for administering PPV for newborn infants.3,4 The ILCOR Neonatal Life Support Task Force used the findings of these systematic reviews to draft treatment recommendations, which were posted online for public comment. The final wording has been published in the Consensus on Science With Treatment Recommendations summary documents from 2021 and 2022.5,6 Full details on the ILCOR systematic review process can be found in the 2022 publication.6 For this 2023 focused update, the Neonatal Life Support writing group analyzed and discussed the systematic reviews, carefully considered the treatment recommendations drafted by the ILCOR Neonatal Life Support Task Force, and incorporated new data published since the systematic reviews were completed. Guideline recommendations were drafted by designated writing group members and then reviewed and refined by all writing group members during regular meetings. The final recommendation wording was reviewed and approved by all writing group members.
Class of Recommendation and Level of Evidence
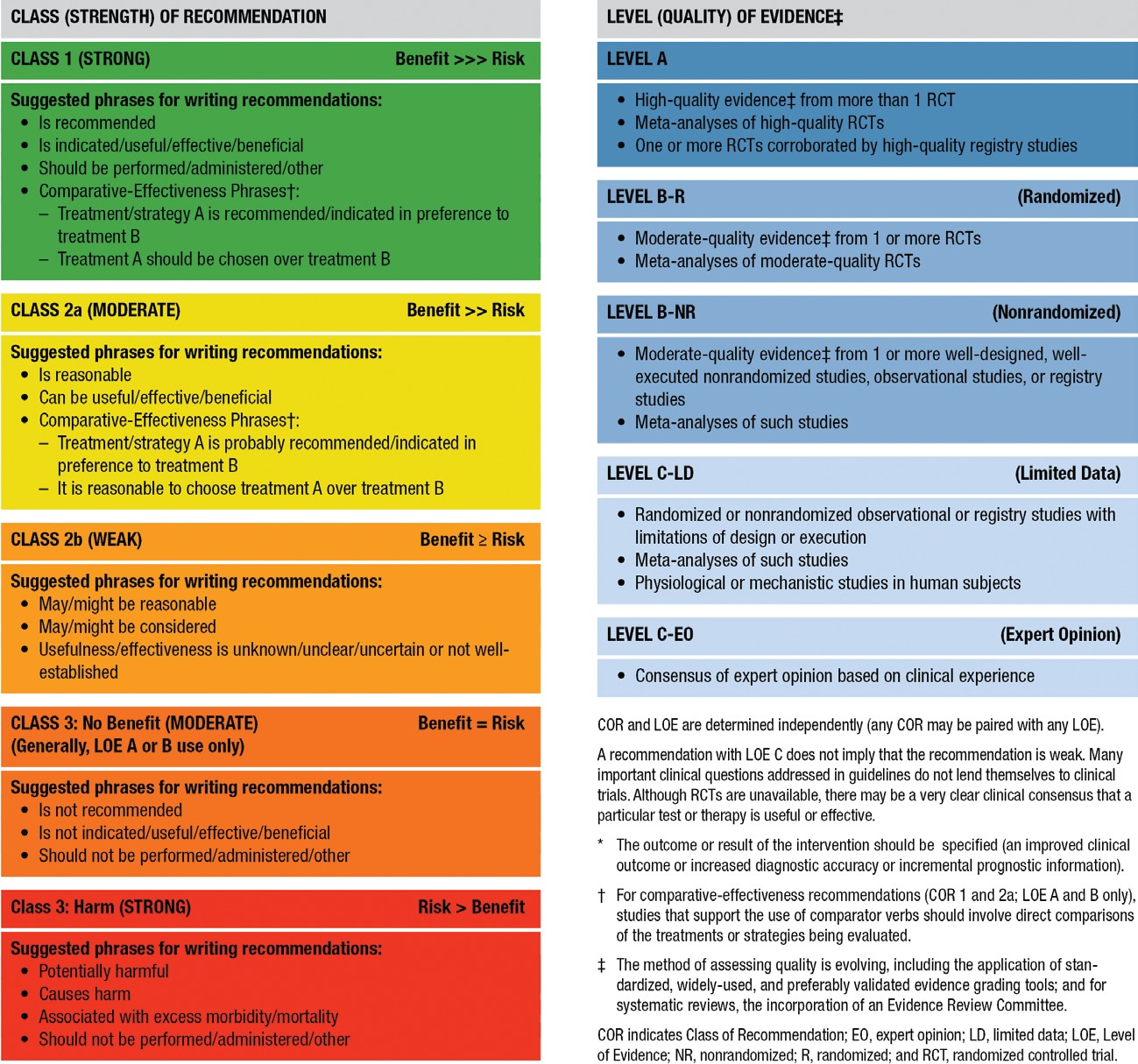
As with all AHA guidelines, each recommendation in this focused update is assigned a Class of Recommendation (COR) on the basis of the strength of the evidence, alternative treatment options, and the effect on patients and society (Table). The Level of Evidence (LOE) is based on the quality, quantity, relevance, and consistency of the available evidence. For each recommendation, the writing group discussed and approved specific wording of recommendations and the COR and LOE assignments. In determining the COR, the writing group considered the LOE and other factors, including systems issues, economic factors, and ethical factors such as equity, acceptability, and feasibility. These evidence review methods, including specific criteria used to determine COR and LOE, are described more fully in “Part 2: Evidence Evaluation and Guidelines Development” of the 2020 guidelines.9 The writing group members had final authority over and formally approved these recommendations.
The overall certainty of the evidence base for neonatal resuscitation science is low. Funding and support for high-certainty clinical trials is a significant need in neonatal resuscitation. Of the 8 recommendations in this focused update, no recommendations are supported by Level A evidence (high-quality evidence from >1 randomized controlled trial [RCT], or ≥1 RCTs corroborated by high-quality registry studies). Five recommendations are supported by Level B-R (randomized) evidence (moderate evidence from ≥1 RCTs) and 1 by Level B-N (nonrandomized) evidence. Two recommendations are based on Level C evidence supported by limited data; no recommendations are based on Level C evidence derived from expert opinion. Likewise, the strength of recommendations is weaker than optimal: no Class 1 (strong) recommendations, 3 Class 2a (moderate) recommendations, 3 Class 2b (weak) recommendations, and 2 Class 3: No Benefit recommendations are included in these guidelines. There are no recommendations designated Class 3: Harm.
Table. Applying the American College of Cardiology/American Heart AssociationClass of Recommendation and Level of Evidence to Clinical Strategies, Interventions, Treatments, or Diagnostic Testing in Patient Care* (Up- dated May 2019)
Guideline Structure
These guidelines are organized into knowledge chunks, grouped into discrete modules of information on specific topics or management issues.9,10 Each modular knowledge chunk includes a table of recommendations that uses the standard AHA nomenclature of COR and LOE. Recommendations are presented in order of COR: most potential benefit (Class 1), followed by lesser certainty of benefit (Class 2), and finally potential for harm or no benefit (Class 3). Following the COR, recommendations are ordered by the certainty of supporting LOE: Level A (high-quality randomized controlled trials) to Level C-EO (expert opinion). A brief introduction puts the recommendations into context with important background information and overarching management or treatment concepts. Recommendation-specific text clarifies the rationale and key study data supporting the recommendations. Hyperlinked references facilitate quick access and review. All writing group members reviewed and approved the final manuscript.
These guidelines were submitted for blinded peer review to 11 subject-matter experts nominated by the AHA and the AAP. Before appointment, all peer reviewers were required to disclose relationships with industry and any other conflicts of interest, and all disclosures were reviewed by AHA staff. Peer reviewer feedback was provided for guidelines in draft format and again in final format. All guidelines were reviewed and approved for publication by the AHA Science Advisory and Coordinating Committee, the AHA Executive Committee, and the AAP Executive Board. Comprehensive disclosure information for peer reviewers is listed in Appendix 2.
These recommendations augment the last full set of AHA recommendations for neonatal resuscitation made in 2020.7 All other recommendations and algorithms published in the 2020 guidelines remain the official recommendations of the AHA Emergency Cardiovascular Care Science Subcommittee and writing groups.
REFERENCES
Gomersall J, Berber S, Middleton P, McDonald SJ, Niermeyer S, El-Naggar W, Davis PG, Schmolzer GM, Ovelman C, Soll RF, et al. Umbilical cord management at term and late preterm birth: a meta-analysis. Pediatrics. 2021;147:e2020015404. doi: 10.1542/peds.2020-015404
Seidler AL, Gyte GML, Rabe H, Diaz-Rossello JL, Duley L, Aziz K, Testoni Costa-Nobre D, Davis PG, Schmolzer GM, Ovelman C, et al. Umbilical cord management for newborns <34 weeks’ gestation: a meta-analysis. Pediatrics. 2021;147:e20200576. doi: 10.1542/peds.2020-0576
Trevisanuto D, Roehr CC, Davis PG, Schmölzer GM, Wyckoff MH, Liley HG, Rabi Y, Weiner GM. Devices for administering ventilation at birth: a systematic review. Pediatrics. 2021;148:e2021050174. doi: 10.1542/peds.2021-050174
Yamada NK, McKinlay CJ, Quek BH, Schmölzer GM, Wyckoff MH, Liley HG, Rabi Y, Weiner GM. Supraglottic airways compared with face masks for neonatal resuscitation: a systematic review. Pediatrics. 2022;150:e2022056568. doi: 10.1542/peds.2022-056568
Wyckoff MH, Singletary EM, Soar J, Olasveengen TM, Greif R, Liley HG, Zideman D, Bhanji F, Andersen LW, Avis SR, et al. 2021 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: summary from the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Circulation. 2022;145:e645–e721. doi: 10.1161/CIR.0000000000001017
Wyckoff MH, Greif R, Morley PT, Ng K-C, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, et al. 2022 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: summary from the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2022;146:e483–e557. doi: 10.1161/CIR.0000000000001095
Aziz K, Lee HC, Escobedo MB, Hoover AV, Kamath-Rayne BD, Kapadia VS, Magid DJ, Niermeyer S, Schmolzer GM, Szyld E, et al. Part 5: neonatal resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S524–S550. doi: 10.1161/CIR.0000000000000902
Wyckoff MH, Wyllie J, Aziz K, de Almeida MF, Fabres J, Fawke J, Guinsburg R, Hosono S, Isayama T, Kapadia VS, et al. Neonatal life support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S185–S221. doi: 10.1161/CIR.0000000000000895
Magid DJ, Aziz K, Cheng A, Hazinski MF, Hoover AV, Mahgoub M, Panchal AR, Sasson C, Topjian AA, Rodriguez AJ, et al. Part 2: evidence evaluation and guidelines development: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142:S358–S365. doi: 10.1161/CIR.0000000000000898
Levine GN, O’Gara PT, Beckman JA, Al-Khatib SM, Birtcher KK, Cigarroa JE, de Las Fuentes L, Deswal A, Fleisher LA, Gentile F, et al. Recent innovations, modifications, and evolution of ACC/AHA clinical practice guidelines: an update for our constituencies: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e879–e886. doi: 10.1161/cir.0000000000000651
Management of the umbilical cord and placental transfusion at delivery remains an area of robust investigation. The volume of blood transferred from the placenta to the newborn infant and the effect of that transfusion vary on the basis of gestational age at delivery, mode of delivery, the time from delivery to cord clamping, any milking of the umbilical cord, and physiological status of the newborn infant.
Both the American College of Obstetrics and Gynecology and the AAP have produced guidelines about umbilical cord management.1,2 The most recent guidance from the AHA was published in 2020 and included all gestational ages and methods of placental transfusion.3 However, the developmental differences between preterm, late preterm, and term infants affect the outcomes of different cord management strategies, including the need for cardiorespiratory support in the delivery room, rate of moderate-to-severe hypoxic-ischemic encephalopathy, hematologic indices, need for admission to the neonatal intensive care unit, and use of therapeutic hypothermia. Because of these variations, ILCOR subsequently performed 2 different systematic reviews for cord management, 1 for late preterm and term infants4 and 1 for preterm infants.5 This focused update provides separate recommendations for these 2 distinct groups and relevant evidence published since those meta-analyses through September 2022.
Recommendations for Term/Late Preterm Newborn Umbilical Cord Management
COR
LOE
Recommendations
2a
B-R
1. For term and late preterm newborn infants ≥34 weeks’ gestation who do not require resuscitation, delayed cord clamping (DCC) (≥30 seconds) can be beneficial when compared to early cord clamping (<30 seconds).
2b
B-R
2. For nonvigorous term and late preterm infants (35–42 weeks’ gestation), intact cord milking may be reasonable when compared to early cord clamping (<30 seconds).
3: No
Benef it
C-LD
3. For term and late preterm newborn infants ≥34 weeks’ gestation who do not require resuscitation, intact cord milking is not known to be beneficial when compared to DCC (≥30 seconds).
Recommendation-Specific Supportive Text
Four RCTs (537 infants) found no difference in mortality between early and late cord clamping for term and late preterm infants.6–9 Low-certainty evidence from 15 studies (2641 infants) shows that DCC results in increased early hematologic indices (either hemoglobin or hematocrit) compared with early cord clamping.7,8,10–22
One RCT including 1730 nonvigorous newborn infants limited to 35 to 42 weeks’ gestation (not including infants 34
weeks’ gestation) comparing intact umbilical cord milking with early cord clamping found no difference in the primary outcome of admission to the neonatal intensive care unit. However, differences in several secondary outcomes (including increased hemoglobin levels and a reduced need for cardiorespiratory support) make umbilical cord milking in this population a reasonable option.23 Additional studies would be helpful in further evaluating this intervention.
There is no evidence available to support intact cord milking compared with DCC in vigorous term and late preterm infants.
Recommendations for Preterm Newborn Umbilical Cord Management
COR
LOE
Recommendations
2a
B-R
1. For preterm newborn infants <34 weeks’ gestation who do not require resuscitation, delaying cord clamping (≥30 seconds) can be beneficial when compared to early cord clamping (<30 seconds).
2b
B-R
2. For preterm newborn infants between 28 and 34 weeks’ gestation who do not require resuscitation and in whom DCC cannot be performed, intact cord milking may be reasonable.
3: No
Benef it
B-R
3. For preterm newborn infants <28 weeks’ gestation, intact cord milking is not recommended.
Recommendation-Specific Supportive Text
Sixteen RCTs (2988 infants) showed possible improvement in survival to discharge for infants receiving DCC compared with early cord clamping. DCC varied from 30 seconds to >2 minutes.24–39 Six studies (351 infants) showed that infants receiving DCC had decreased inotrope use in the first 24 hours.33,36–38,40,41 Infants receiving DCC had improved hematologic indices within 24 hours and 7 days,24–27,31–43 and received fewer red blood cell transfusions during admission.24,27,28,32,35,37–40,42–44
Intact cord milking a.
Versus early cord clamping: In 11 trials (983 infants), infants receiving intact cord milking had higher hematologic indices in the first 24 hours.43,45–55 In 5 trials (439 infants), infants receiving intact cord milking received fewer inotropes in the first 24 hours.45–47,49,55 In infants 28 to 32 weeks’ gestation, 10 studies (889 infants) could not exclude benefit or harm of intact cord milking for severe intraventricular hemorrhage.43,45–47,49,51–53,55,56
b.
Versus DCC: A single trial including 292 preterm infants (28–31+6/7 weeks’ gestation) showed no increased risk of
severe intraventricular hemorrhage for umbilical cord milking compared with DCC.57
In a single study of 182 infants born 23 to 27+6/7 weeks’ gestation not requiring resuscitation, severe intraventricular hemorrhage was significantly higher in those who received umbilical cord milking compared with DCC.57
American Academy of Pediatrics. Delayed umbilical cord clamping after birth. Pediatrics. 2017;139:e2017095. doi: 10.1542/peds.2017-0957
Aziz K, Lee HC, Escobedo MB, Hoover AV, Kamath-Rayne BD, Kapadia VS, Magid DJ, Niermeyer S, Schmolzer GM, Szyld E, et al. Part 5: neonatal resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary -Resuscitation and Emergency -Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S524–S550. doi: 10.1161/CIR.0000000000000902
Gomersall J, Berber S, Middleton P, McDonald SJ, Niermeyer S, El-Naggar W, Davis PG, Schmolzer GM, Ovelman C, Soll RF, et al. Umbilical cord management at term and late preterm birth: a meta-analysis. Pediatrics. 2021;147:e2020015404. doi: 10.1542/peds.2020-015404
Seidler AL, Gyte GML, Rabe H, Diaz-Rossello JL, Duley L, Aziz K, Testoni Costa-Nobre D, Davis PG, Schmolzer GM, Ovelman C, et al. Umbilical cord management for newborns <34 weeks’ gestation: a meta-analysis. Pediatrics. 2021;147:e20200576. doi: 10.1542/peds.2020-0576
Backes CH, Huang H, Cua CL, Garg V, Smith CV, Yin H, Galantowicz M, Bauer JA, Hoffman TM. Early versus delayed umbilical cord clamping in infants with congenital heart disease: a pilot, randomized, controlled trial. J Perinatol. 2015;35:826–831. doi: 10.1038/jp.2015.89
Ceriani Cernadas JM, Carroli G, Pellegrini L, Otano L, Ferreira M, Ricci C, Casas O, Giordano D, Lardizabal J. The effect of timing of cord clamping on neonatal venous hematocrit values and clinical outcome at term: a randomized, controlled trial. Pediatrics. 2006;117:e779–e786. doi: 10.1542/peds.2005-1156
Chopra A, Thakur A, Garg P, Kler N, Gujral K. Early versus delayed cord clamping in small for gestational age infants and iron stores at 3 months of age: a randomized controlled trial. BMC Pediatr. 2018;18:234. doi: 10.1186/s12887-018-1214-8
Datta BV, Kumar A, Yadav R. A randomized controlled trial to evaluate the role of brief delay in cord clamping in preterm neonates (34–36 weeks) on short-term neurobehavioural outcome. J Trop Pediatr. 2017;63:418–424. doi: 10.1093/tropej/fmx004
Al-Tawil MM, Abdel-Aal MR, Kaddah MA. A randomized controlled trial on delayed cord clamping and iron status at 3–5 months in term neonates held at the level of maternal pelvis. J Neonatal-Perinat Med. 2012;5:319–326. doi: 10.3233/npm-1263112
Chaparro CM, Neufeld LM, Tena Alavez G, Eguia-Liz Cedillo R, Dewey KG. Effect of timing of umbilical cord clamping on iron status in Mexican infants: a randomised controlled trial. Lancet. 2006;367:1997–2004. doi: 10.1016/S0140-6736(06)68889-2
Chen X, Li X, Chang Y, Li W, Cui H. Effect and safety of timing of cord clamping on neonatal hematocrit values and clinical outcomes in term infants: a randomized controlled trial. J Perinatol. 2018;38:251–257. doi: 10.1038/s41372-017-0001-y
De Paco C, Herrera J, Garcia C, Corbalán S, Arteaga A, Pertegal M, Checa R, Prieto MT, Nieto A, Delgado JL. Effects of delayed cord clamping on the third stage of labour, maternal haematological parameters and acid-base status in fetuses at term. Eur J Obstet Gynecol Reprod Biol. 2016;207:153–156. doi: 10.1016/j.ejogrb.2016.10.031
Emhamed MO, van Rheenen P, Brabin BJ. The early effects of delayed cord clamping in term infants born to Libyan mothers.
Fawzy AE-MA, Moustafa , El-Kassar AA, El-Kassar YS, Swelem MS, El-Agwany AS, Diab DA. Early versus delayed cord clamping of term births in Shatby Maternity University Hospital. Prog Obstet Ginecol. 2015;58:389–392. doi: 10.1016/j.pog.2015.05.001
Jahazi A, Kordi M, Mirbehbahani NB, Mazloom SR. The effect of early and late umbilical cord clamping on neonatal hematocrit.
Mohammad K, Tailakh S, Fram K, Creedy D. Effects of early umbilical cord clamping versus delayed clamping on maternal and neonatal outcomes: a Jordanian study. J Matern Fetal Neonatal Med. 2021;34:231–237. doi: 10.1080/14767058.2019.1602603
Philip AG. Further observations on placental transfusion. Obstet Gynecol. 1973;42:334–343.
Salari Z, Rezapour M, Khalili N. Late umbilical cord clamping, neonatal hematocrit and Apgar scores: a randomized controlled trial. J Neonatal Perinatal Med. 2014;7:287–291. doi: 10.3233/NPM-1463913
Ultee CA, van der Deure J, Swart J, Lasham C, van Baar AL. Delayed cord clamping in preterm infants delivered at 34–36 weeks’
Vural I, Ozdemir H, Teker G, Yoldemir T, Bilgen H, Ozek E. Delayed cord clamping in term large-for-gestational age infants: a prospective randomised study. J Paediatr Child Health. 2019;55:555–560. doi: 10.1111/jpc.14242
Yadav AK, Upadhyay A, Gothwal S, Dubey K, Mandal U, Yadav CP. Comparison of three types of intervention to enhance placental redistribution in term newborns: randomized control trial. J Perinatol. 2015;35:720–724. doi: 10.1038/jp.2015.65
Katheria AC, Clark E, Yoder B, Schmolzer GM, Yan Law BH, El-Naggar W, Rittenberg D, Sheth S, Mohamed MA, Martin C, et al. Umbilical cord milking in nonvigorous infants: a cluster-randomized crossover trial. Am J Obstet Gynecol. 2023;228:217.e1–217.e14. doi: 10.1016/j.ajog.2022.08.015
Armanian AM, Tehrani HG, Ansari M, Ghaemi S. Is “delayed umbilical cord clamping” beneficial for premature newborns?. Int J Pediatr. 2017;5:4909–4918. doi: 10.22038/ijp.2016.7909
Backes CH, Huang H, Iams JD, Bauer JA, Giannone PJ. Timing of umbilical cord clamping among infants born at 22 through 27
Baenziger O, Stolkin F, Keel M, von Siebenthal K, Fauchere JC, Das Kundu S, Dietz V, Bucher HU, Wolf M. The influence of the timing of cord clamping on postnatal cerebral oxygenation in preterm neonates: a randomized, controlled trial. Pediatrics. 2007;119:455–459. doi: 10.1542/peds.2006-2725
Das B, Sundaram V, Kumar P, Mordi WT, Dhaliwal LK, Das R. Effect of placental transfusion on iron stores in moderately preterm neonates of 30–33 weeks gestation. Indian J Pediatr. 2018;85:172–178. doi: 10.1007/s12098-017-2490-2
Duley L, Dorling J, Pushpa-Rajah A, Oddie SJ, Yoxall CW, Schoonakker B, Bradshaw L, Mitchell EJ, Fawke JA, Cord Pilot Trial Collaborative Group. Randomised trial of cord clamping and initial stabilisation at very preterm birth. Arch Dis Child Fetal Neonatal Ed. 2018;103:F6–F14. doi: 10.1136/archdischild-2016-312567
Hofmeyr GJ, Bolton KD, Bowen DC, Govan JJ. Periventricular/intraventricular haemorrhage and umbilical cord clamping. Findings and hypothesis. S Afr Med J. 1988;73:104–106.
Hofmeyr GJ, Gobetz L, Bex PJ, Van der Griendt M, Nikodem C, Skapinker R, Delahunt T. Periventricular/intraventricular hemorrhage following early and delayed umbilical cord clamping. A randomized controlled trial. Online J Curr Clin Trials. 1993;Doc No 110.
Kinmond S, Aitchison TC, Holland BM, Jones JG, Turner TL, Wardrop CA. Umbilical cord clamping and preterm infants: a randomised trial. BMJ. 1993;306:172–175. doi: 10.1136/bmj.306.6871.172
Kugelman A, Borenstein-Levin L, Riskin A, Chistyakov I, Ohel G, Gonen R, Bader D. Immediate versus delayed umbilical cord clamping in premature neonates born <35 weeks: a prospective, randomized, controlled study. Am J Perinatol. 2007;24:307–315. doi: 10.1055/s-2007-981434
McDonnell M, Henderson-Smart DJ. Delayed umbilical cord clamping in preterm infants: a feasibility study. J Paediatr Child Health. 1997;33:308–310. doi: 10.1111/j.1440-1754.1997.tb01606.x
Mercer JS, McGrath MM, Hensman A, Silver H, Oh W. Immediate and delayed cord clamping in infants born between 24 and 32 weeks: a pilot randomized controlled trial. J Perinatol. 2003;23:466–472. doi: 10.1038/sj.jp.7210970
Mercer JS, Vohr BR, Erickson-Owens DA, Padbury JF, Oh W. Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J Perinatol. 2010;30:11–16. doi: 10.1038/jp.2009.170
Oh W, Fanaroff AA, Carlo WA, Donovan EF, McDonald SA, Poole WK. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Effects of delayed cord clamping in very-low-birth-weight infants. J Perinatol. 2011;31(suppl 1):S68–S71. doi: 10.1038/jp.2010.186
Rabe H, Wacker A, Hulskamp G, Hornig-Franz I, Schulze-Everding A, Harms E, Cirkel U, Louwen F, Witteler R, Schneider HP. A randomised controlled trial of delayed cord clamping in very low birth weight preterm infants. Eur J Pediatr. 2000;159:775–777. doi: 10.1007/pl00008345
Ruangkit C, Bumrungphuet S, Panburana P, Khositseth A, Nuntnarumit P. A randomized controlled trial of immediate versus delayed umbilical cord clamping in multiple-birth infants born preterm. Neonatology. 2019;115:156–163. doi: 10.1159/000494132
Tarnow-Mordi W, Morris J, Kirby A, Robledo K, Askie L, Brown R, Evans N, Finlayson S, Fogarty M, Gebski V, et al. Delayed versus immediate cord clamping in preterm infants. N Engl J Med. 2017;377:2445–2455. doi: 10.1056/NEJMoa1711281
Dong XY, Sun XF, Li MM, Yu ZB, Han SP. Influence of delayed cord clamping on preterm infants with a gestational age of <32
weeks [in Chinese]. Zhongguo Dang Dai Er Ke Za Zhi. 2016;18:635–638. doi: 10.7499/j.issn.1008-8830.2016.07.013
Gokmen Z, Ozkiraz S, Tarcan A, Kozanoglu I, Ozcimen EE, Ozbek N. Effects of delayed umbilical cord clamping on peripheral blood hematopoietic stem cells in premature neonates. J Perinat Med. 2011;39:323–329. doi: 10.1515/jpm.2011.021
Dipak NK, Nanavat RN, Kabra NK, Srinivasan A, Ananthan A. Effect of delayed cord clamping on hematocrit, and thermal and hemodynamic stability in preterm neonates: a randomized controlled trial. Indian Pediatr. 2017;54:112–115. doi: 10.1007/s13312-017-1011-8
Finn D, Ryan DH, Pavel A, O’Toole JM, Livingstone V, Boylan GB, Kenny LC, Dempsey EM. Clamping the umbilical cord in premature deliveries
(CUPiD): neuromonitoring in the immediate newborn period in a randomized, controlled trial of preterm infants born at <32
weeks of gestation. J Pediatr. 2019;208:121–126.e122. doi: 10.1016/j.jpeds.2018.12.039
Rana A, Agarwal K, Ramji S, Gandhi G, Sahu L. Safety of delayed umbilical cord clamping in preterm neonates of less than 34 weeks of gestation: a randomized controlled trial. Obstet Gynecol Sci. 2018;61:655–661. doi: 10.5468/ogs.2018.61.6.655
Elimian A, Goodman J, Escobedo M, Nightingale L, Knudtson E, Williams M. Immediate compared with delayed cord clamping in the preterm neonate: a randomized controlled trial. Obstet Gynecol. 2014;124:1075–1079. doi: 10.1097/AOG.0000000000000556
El-Naggar W, Simpson D, Hussain A, Armson A, Dodds L, Warren A, Whyte R, McMillan D. Cord milking versus immediate clamping in preterm infants: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2019;104:F145–F150. doi: 10.1136/archdischild-2018-314757
Hosono S, Mugishima H, Fujita H, Hosono A, Minato M, Okada T, Takahashi S, Harada K. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks’ gestation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2008;93:F14–F19. doi: 10.1136/adc.2006.108902
Katheria A, Blank D, Rich W, Finer N. Umbilical cord milking improves transition in premature infants at birth. PLoS One. 2014;9:e94085. doi: 10.1371/journal.pone.0094085
Katheria AC, Leone TA, Woelkers D, Garey DM, Rich W, Finer NN. The effects of umbilical cord milking on hemodynamics and neonatal outcomes in premature neonates. J Pediatr. 2014;164:1045–1050.e1. doi: 10.1016/j.jpeds.2014.01.024
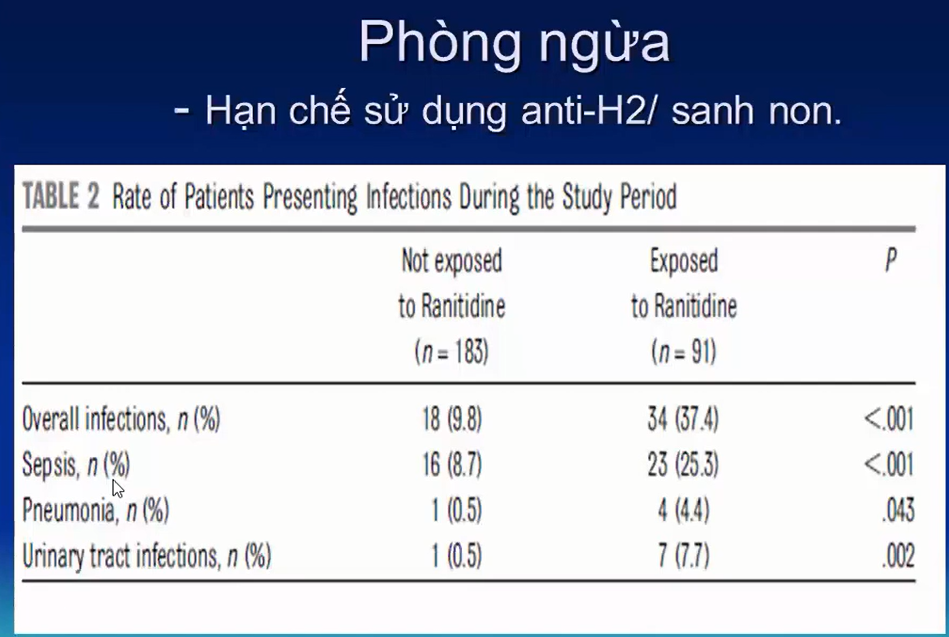
Li J, Yu B, Wang W, Luo D, Dai QL, Gan XQ. Does intact umbilical cord milking increase infection rates in preterm infants with premature prolonged rupture of membranes?. J Matern Fetal Neonatal Med. 2020;33:184–190. doi: 10.1080/14767058.2018.1487947
March MI, Hacker MR, Parson AW, Modest AM, de Veciana M. The effects of umbilical cord milking in extremely preterm infants: a randomized controlled trial. J Perinatol. 2013;33:763–767. doi: 10.1038/jp.2013.70
Mercer JS, Erickson-Owens DA, Vohr BR, Tucker RJ, Parker AB, Oh W, Padbury JF. Effects of placental transfusion on neonatal and 18 month outcomes in preterm infants: a randomized controlled trial. J Pediatr. 2016;168:50–55.e51. doi: 10.1016/j.jpeds.2015.09.068
Silahli M, Duman E, Gokmen Z, Toprak E, Gokdemir M, Ecevit A. The relationship between placental transfusion, and thymic size and neonatal morbidities in premature infants: a randomized control trial. J Pakistan Med Assoc. 2018;68:1560–1565.
Song SY, Kim Y, Kang BH, Yoo HJ, Lee M. Safety of umbilical cord milking in very preterm neonates: a randomized controlled study. Obstet Gynecol Sci. 2017;60:527–534. doi: 10.5468/ogs.2017.60.6.527
Alan S, Arsan S, Okulu E, Akin IM, Kilic A, Taskin S, Cetinkaya E, Erdeve O, Atasay B. Effects of umbilical cord milking on the need for packed red blood cell transfusions and early neonatal hemodynamic adaptation in preterm infants born ≤1500 g: a prospective, randomized, controlled trial. J Pediatr Hematol Oncol. 2014;36:e493–e498. doi: 10.1097/MPH.0000000000000143
Katheria A, Reister F, Essers J, Mendler M, Hummler H, Subramaniam A, Carlo W, Tita A, Truong G, Davis-Nelson S, et al. Association of umbilical cord milking vs delayed umbilical cord clamping with death or severe intraventricular hemorrhage among preterm infants. JAMA. 2019;322:1877–1886. doi: 10.1001/jama.2019.16004
VENTILATORY SUPPORT AFTER BIRTH: DEVICES AND INTERFACES TO ADMINISTER PPV
Background
The 2020 AHA guidelines provided recommendations for when and how to provide PPV, including guidance for
-inflation pressures, the use of positive end-expiratory pressure, ventilation rate, and inspiratory time.1 The recommendations provided in this focused update discuss devices to deliver PPV, and the choice between a face mask and a supraglottic airway as the interface used for PPV.
Several devices are available to administer PPV, including self-inflating bags, flow-inflating bags, and T-piece resuscitators. The choice of PPV device depends on factors reflecting the context at a birthing site: the number of births, the case mix, availability of a compressed gas source, familiarity with the different devices, amount of training required to use each device, and device cost. Because both T-piece resuscitators and flow-inflating bags require a compressed gas source to function, a self-inflating bag should be available as a backup in the event of compressed gas failure when using either of these devices.
Available interfaces for PPV delivery include face masks, nasal prongs, and supraglottic airways. This focused update specifically addresses the choice between face masks and supraglottic airways as the primary interface during PPV.
Recommendations for Devices Used to Administer PPV for Newborn Infants
COR
LOE
Recommendations
2a
B-NR
1. It can be beneficial to use a T-piece resuscitator instead of a self-inflating bag, with or without a positive
end-expiratory pressure valve, for administering positive-pressure ventilation to newborn infants, particularly for preterm infants.
Recommendation-Specific Supportive Text
A meta-analysis of 4 RCTs (1247 term and preterm infants) found that resuscitation with a T-piece resuscitator compared with a self-inflating bag reduced the duration of PPV and decreased risk of bronchopulmonary dysplasia.2 Although subgroup analyses by gestational age were not feasible in this meta-analysis, bronchopulmonary dysplasia is an outcome that affects preterm infants, and the use of a T-piece resuscitator may present the greatest benefit to preterm infants. The systematic review did not identify any studies that evaluated the use of flow-inflating bags.2
Recommendation for Interfaces Used to Administer PPV for Newborn Infants
COR
LOE
Recommendation
2b
C-LD
1. It may be reasonable to use a supraglottic airway as the primary interface to administer PPV instead of a face mask for newborn infants delivered at
≥34 0/7 weeks’ gestation.
Recommendation-Specific Supportive Text
1. A meta-analysis of 6 RCTs (1823 infants delivered at ≥34 0/7 weeks’ gestation) found that use of a supraglottic airway decreased the probability of failure to improve with the assigned device, and the rate of endotracheal intubation in the delivery room.3 Failure to improve with the assigned device was a pragmatic outcome chosen to assess whether primary use of the supraglottic airway or face mask to provide PPV led to improvement of neonates undergoing resuscitation after birth. The duration of PPV and time until heart rate reached >100/min were also shorter with the supraglottic airway.
Based on available evidence, this recommendation is limited to newborn infants ≥34 0/7 weeks’ gestation. All studies included in this meta-analysis were performed in lower-resourced settings. No studies have compared face masks with supraglottic devices for initiating PPV during neonatal resuscitation in high-resourced settings. As a result, the effect size reported in this meta-analysis may not be generalizable to settings with greater availability of health care practitioners with advanced skills and highly trained neonatal resuscitation teams.
REFERENCES
Aziz K, Lee HC, Escobedo MB, Hoover AV, Kamath-Rayne BD, Kapadia VS, Magid DJ, Niermeyer S, Schmolzer GM, Szyld E, et al. Part 5: neonatal resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S524–S550. doi: 10.1161/CIR.0000000000000902
Trevisanuto D, Roehr CC, Davis PG, Schmölzer GM, Wyckoff MH, Liley HG, Rabi Y, Weiner GM. Devices for administering ventilation at birth: a systematic review. Pediatrics. 2021;148:e2021050174, doi: 10.1542/peds.2021-050174
Yamada NK, McKinlay CJ, Quek BH, Schmölzer GM, Wyckoff MH, Liley HG, Rabi Y, Weiner GM. Supraglottic airways compared with face masks for neonatal resuscitation: a systematic review. Pediatrics. 2022;150:e2022056568. doi: 10.1542/peds.2022-056568
KNOWLEDGE GAPS AND PRIORITIES OF RESEARCH ACKNOWLEDGMENTS
This focused update is limited to a review of the science on umbilical cord management in term, late preterm, and preterm newborn infants and on the devices and interfaces used for administering PPV during resuscitation of newborn infants. The topics in the knowledge chunks of this update contain additional questions and practices for which evidence was weak, uncertain, or absent. In addition, the following knowledge gaps require further research:
Umbilical Cord Management
Optimal management of the umbilical cord in term, late preterm, and preterm infants who require resuscitation at
delivery
Longer-term outcome data, such as anemia during infancy and neurodevelopmental outcomes, for all umbilical cord management strategies
Devices for Administering PPV
Cost-effectiveness of a T-piece resuscitator compared with a self-inflating bag
The effect of a self-inflating bag with a positive end-expiratory pressure valve on outcomes in preterm newborn infants
Comparison of either a T-piece resuscitator or a self-inflating bag with a flow-inflating bag for administering PPV
Comparison of clinical outcomes by gestational age for any PPV device
Interfaces for Administering PPV
Comparison of supraglottic airway devices and face masks as the primary interface for PPV in high-resourced settings
The amount and type of training required for successful supraglottic airway insertion and the potential for skill decay
The utility of supraglottic airway devices for suctioning secretions from the airway
The efficacy of a supraglottic airway during advanced neonatal resuscitation requiring chest compressions or the
The American Heart Association and the American Academy of Pediatrics make every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This focused update was approved by the American Heart Association Science Advisory and Coordinating Committee on July 15, 2023; the American Heart Association Executive Committee on August 4, 2023; and the American Academy of Pediatrics on July 6, 2023.
This article has been copublished in Circulation.
The expert peer review of AHA-commissioned documents (eg, scientific statements, clinical practice guidelines, systematic reviews) is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit https://professional.heart.org/statements. Select the “Guidelines & Statements” drop-down menu, then click “Publication Development.”
Disclosures
Appendix 1. Writing Group Disclosures
Writing group member
Employment
Research grant
Other research support
Speakers’ bureau/honora ria
Expert witness
Ownership interest
Consultant/ advisory board
Other
Henry C. Lee
University of California San Diego
None
None
None
None
None
None
None
Edgardo Szyld
Indiana University
None
None
None
None
None
None
None
Emer Finan
Mount Sinai Hospital; University of Toronto
None
None
None
None
None
None
None
Jessica L. Illuzzi
Yale School of Medicine
None
None
None
None
None
None
None
Beena D. Kamath-Rayne
American Academy of Pediatrics
None
None
None
None
None
None
Cerebral Palsy Alliance Research Foundation*
Vishal S. Kapadia
UT Southwestern
NIH†
Masimo Corporation†
None
None
None
None
None
None
Susan Niermeyer
University of Colorado
NIH*
None
None
None
None
None
None
Georg M. Schmölzer
University of Alberta
CIHR Grant† CIHR Grant†
None
None
None
None
None
None
Marya L. Strand
Akron Children’s
Hospital
None
None
None
None
None
None
None
Gary M. Weiner
University of Michigan
None
None
None
None
None
None
None
Amanda Williams
Cedars Sinai
None
None
None
None
None
None
None
Myra H. Wyckoff
UT Southwestern
None
None
None
None
None
None
None
Nicole K. Yamada
Stanford University
AHRQ†; AHRQ*
None
None
None
None
None
None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $5000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $5000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
The Ohio State University, Nationwide Children’s Hospital
None
None
None
None
None
None
None
Justin Goldstein
Beth Israel Deaconess Medical Center
None
None
None
None
None
None
None
Arun Gupta
Lucile Packard Children’s Hospital at Stanford University
None
None
None
None
None
None
None
Lia Lowrie
St. Louis University School of Medicine
None
None
None
None
None
None
None
Allison Markowsky
Children’s National
Hospital
None
None
None
None
None
None
None
Saurabhkumar
C. Patel
University of Illinois Chicago
None
None
None
None
None
None
None
Betsy Peterson
SOAPM
None
None
None
None
None
None
None
Clara Song
Kaiser Permanente
None
None
None
None
None
None
None
Michael R. Stenger
The Ohio State
-University
None
None
None
None
None
None
None
Muhammad Waseem
Lincoln Medical Center
None
None
None
None
None
None
None
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $5000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $5000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
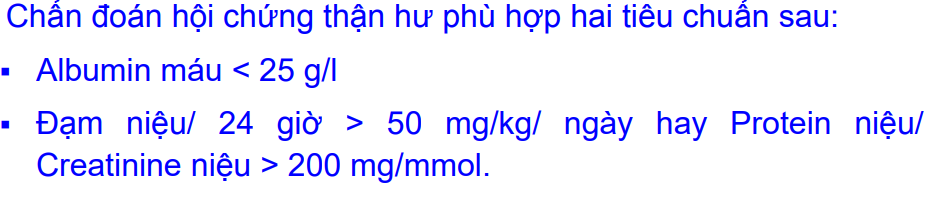
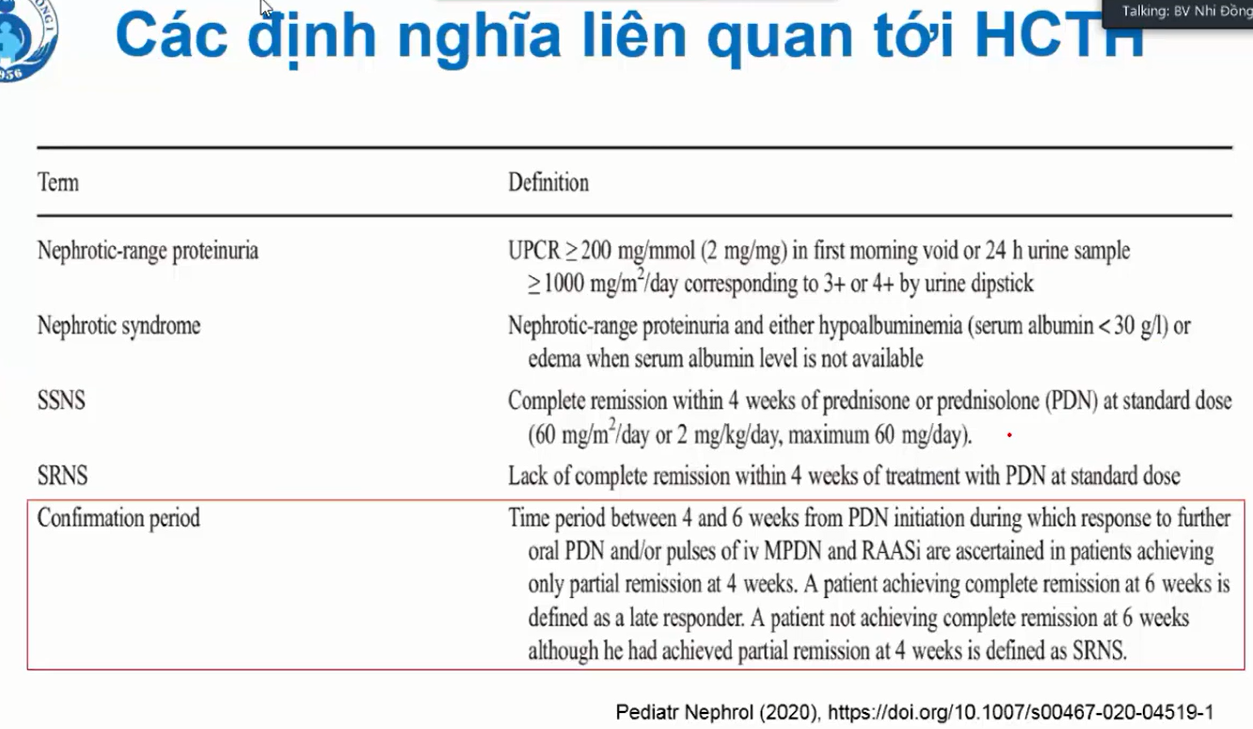
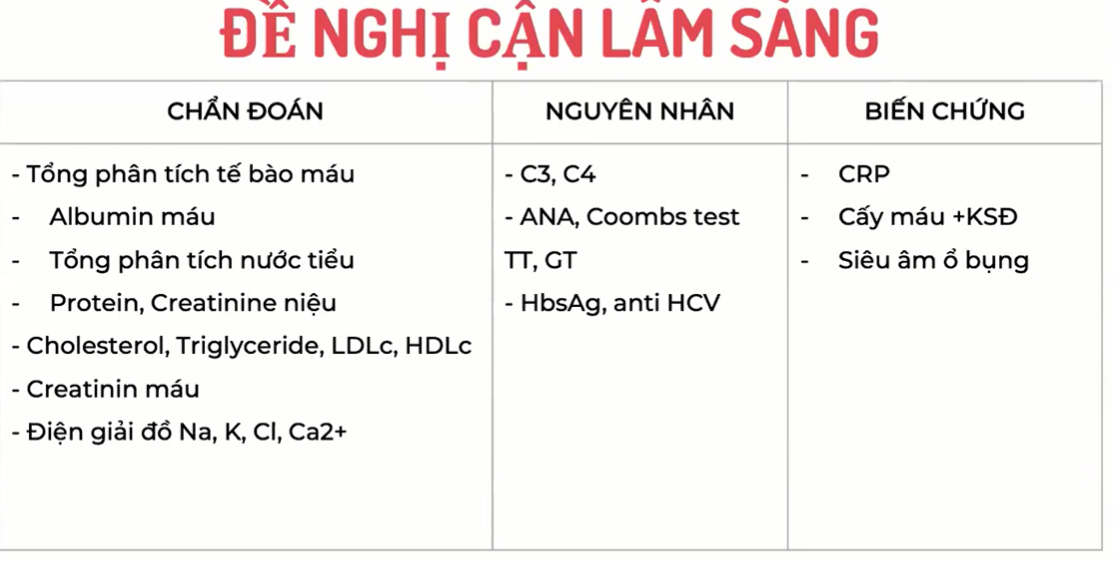
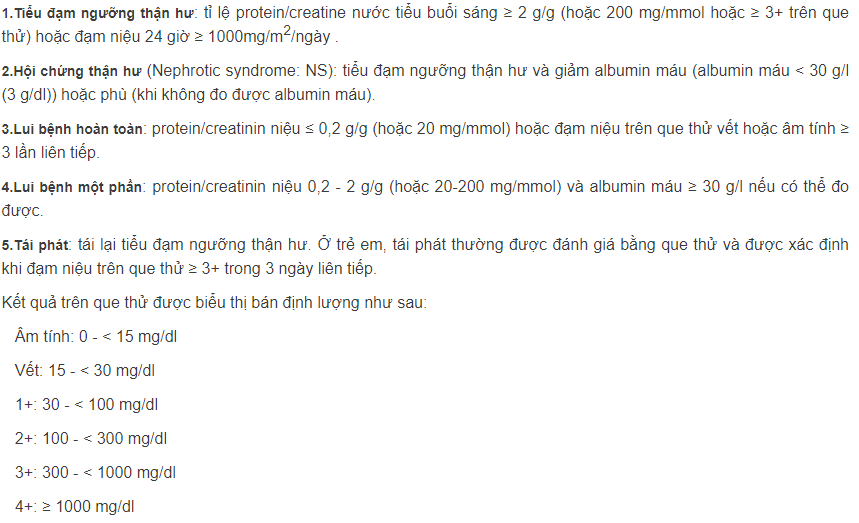
*Cholesterol, Triglyceride => tiêu chuẩn chẩn đoán hiện tại không còn dùng Cholesterol và triglycerite máu nữa
*XN chẩn đoán nguyên nhân giờ không cần thiết nữa
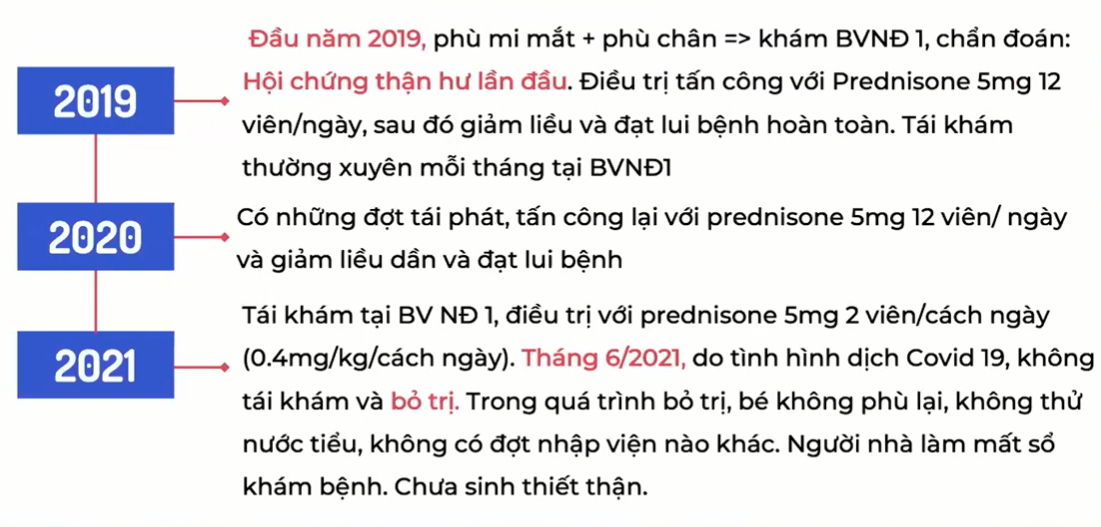
– Bé này được chẩn đoán cort từ lúc 8 tuổi ( trẻ từ 1 – 10 tuổi thì 90% là HCTH nguyên phát)
-Thường HCTH thứ phát thường kém đáp ứng với cort => Bé này lại nhạy với cort do từ trước giờ điều trị chỉ dùng cort, đã có đợt được ngưng thuốc
-Bé này mặc dù tái phát, nhưng tái phát không thường xuyên => nghĩ nghĩ nhiều sẽ nhạy cort
=> HCTH chẩn đoán lần đầu nên làm => những trẻ HCTH khởi phát sau 10 tuổi, thường là HCTH thứ phát => Phải làm CLS để loại trừ lupus ( vì vẫn có thể lupus chir co biểu hiện tại thận): C3, C4, ANA
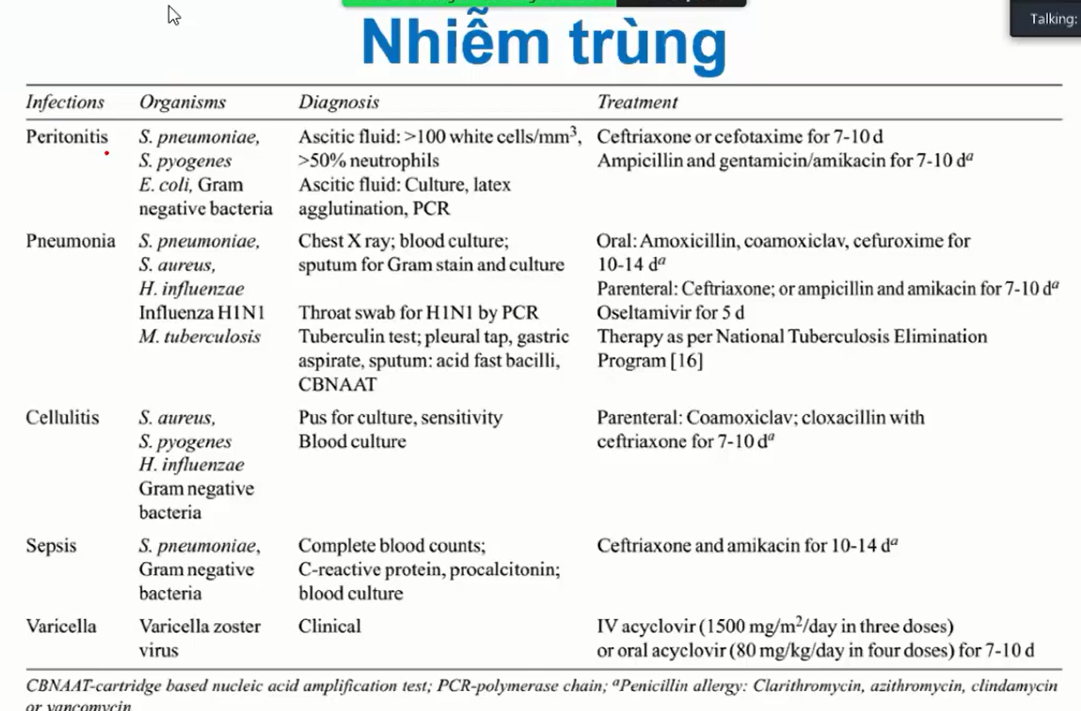
*CRP + CTM: Hiện vẫn chưa loại trừ VPM thứ phát => nên làm Bilan nhiễm trùng
*Cấy máu => Giúp ích nếu dịch màng bụng cấy không ra thì cấy máu cũng giúp chọn kháng sinh
*Siêu âm: Thấy hình ảnh ruột thừa viêm, vỡ, thấy dấu màng cửa, hơi tự do dưới gan…
-HCTH kháng cort: nên làm để quyết định điều trị lipid máu hay không
-HCTH tái phát: thường Cholesterol chỉ tăng trong giai đoạn cấp, nên tái phát xa không làm cũng được
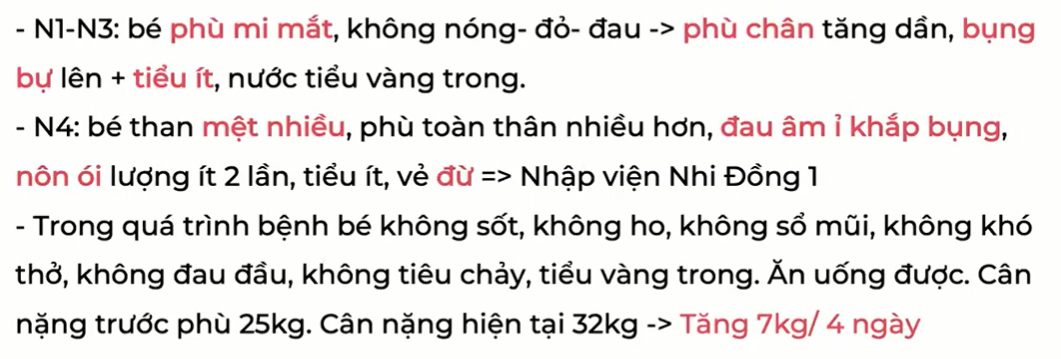
1/ Do bé này đã được chẩn đoán HCTH từ trước, giờ phù lại => nghĩ HCTH tái phát
*Hỏi:
-HCTH đợt trước điều tị đã ổn định chưa ?
-Đợt này phù có nghĩ do nguyên nhân khác/ một bé HCTH đã lui bệnh rồi không ? (vì HCTH có thể đáp ứng điều trị và hồi phục hoàn toàn)
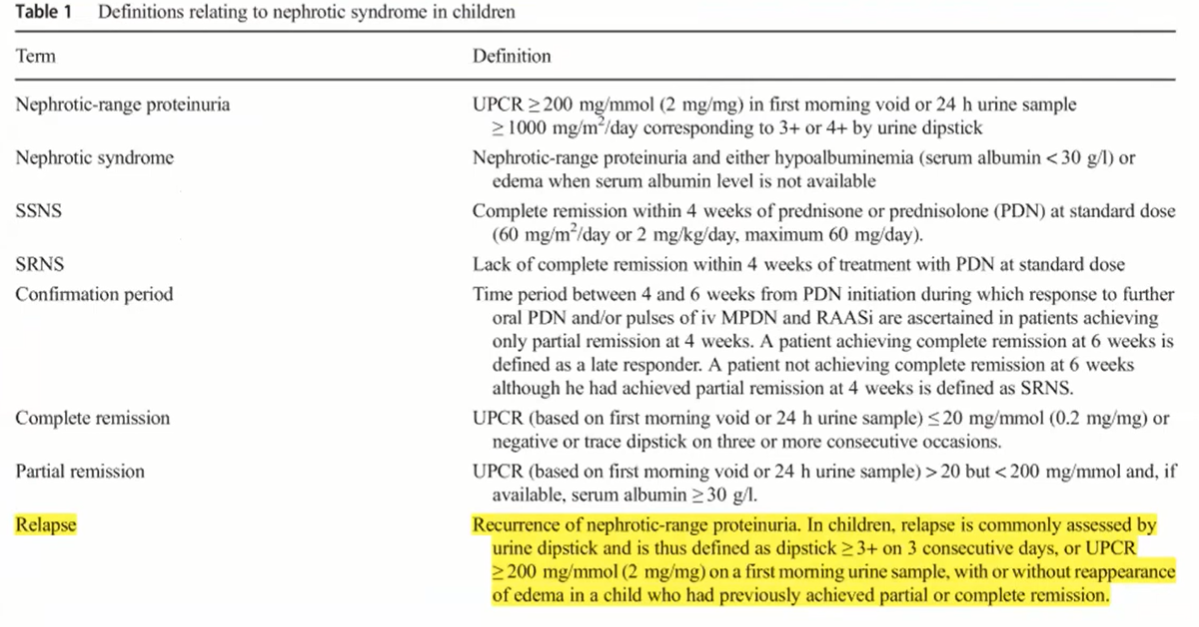
=> Một BN điều đang điều trị cort hoặc đang giảm liều mà phù lại/tiểu đạm ngưỡng thận hư lại thì mới chắc chắn tái phát
Bé này phải khám kĩ để loại trừ phù do nguyên nhân khác
Phù khu trú:
Phù toàn thân: do tim( suy tim phải hoặc suy tim toàn bộ), do gan (HC tăng áp lực TM cửa và HC suy TB gan), do suy dinh dưỡng ( chế độ ăn, tiền căn cắt ruột…)
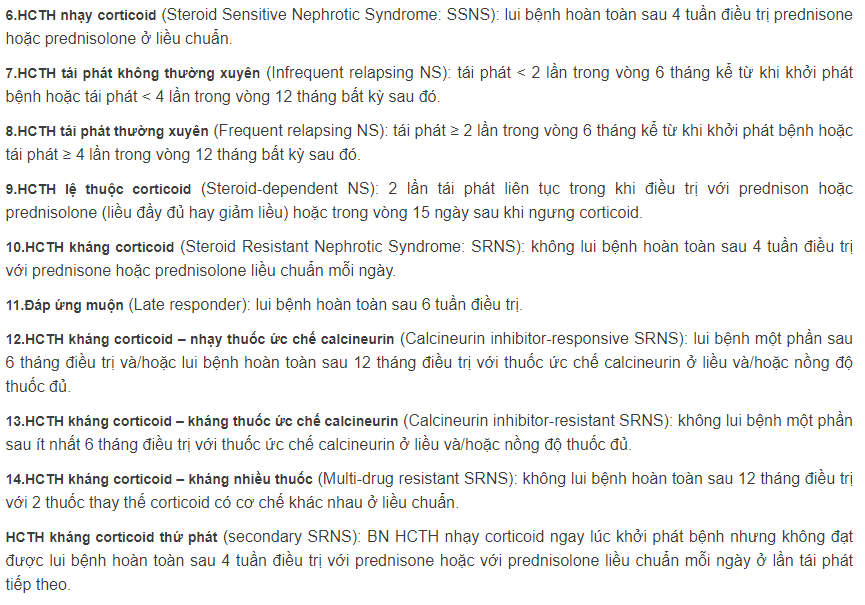
2/ Phân loại HCTH ở bé này
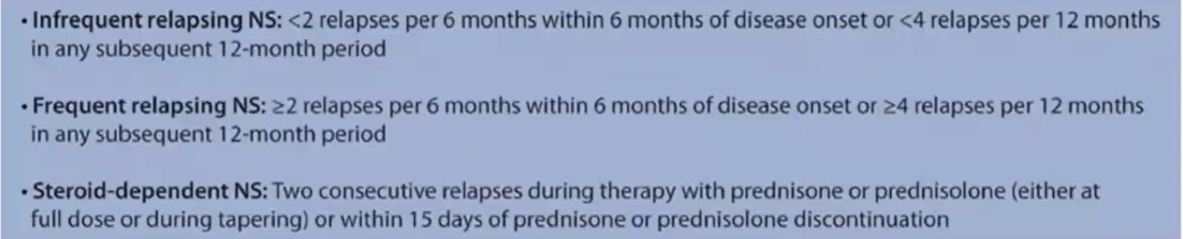
-Tái phát
+Thường xuyên
+Xa ( => Bé này trong suốt quá trình điều trị chỉ sử dụng cort, có những thời điểm đã được ngưng cort => HCTH nhạy với cort. Suốt 8 tháng ngưng thuốc, nay mới ghi nhận triệu chứng phù lại => tái phát xa
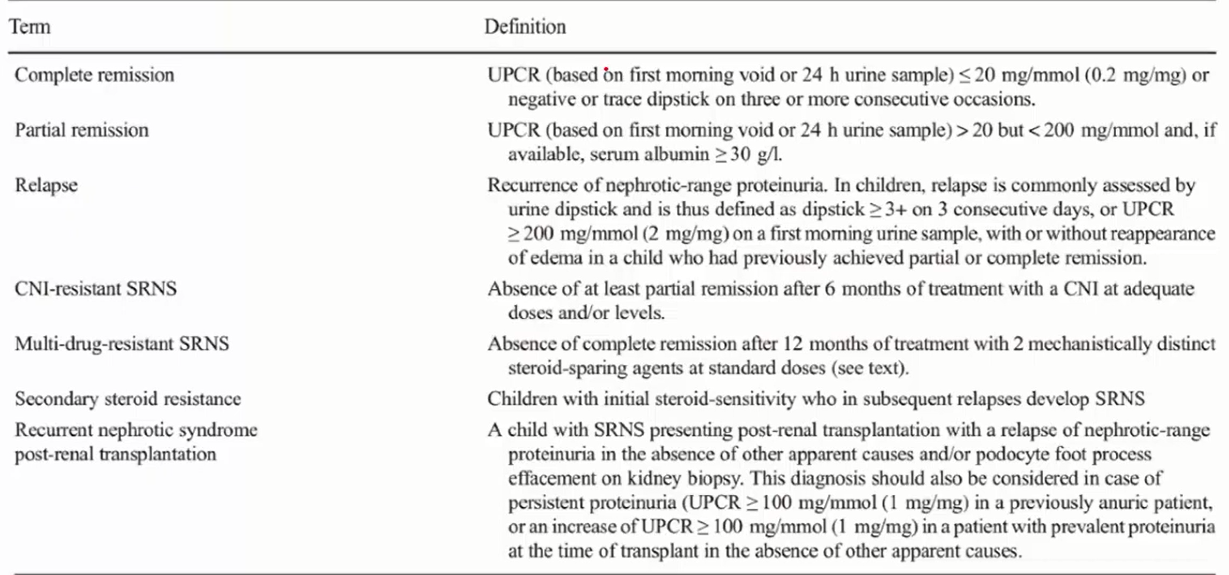
-Kháng cort
-Lệ thuộc cort
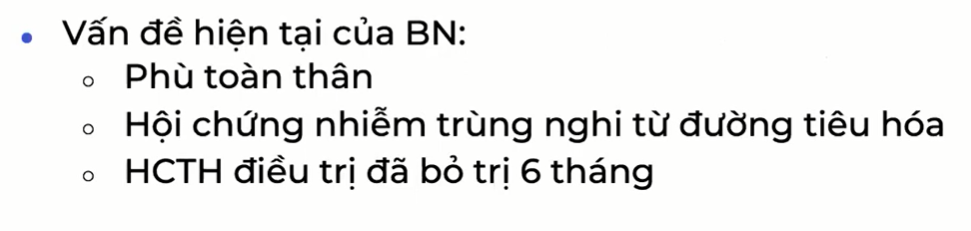
3/ Vấn đề hiện tại
*Quan tâm
-Sốt
-Nôn ói
-Tiêu lỏng
-Bụng
+Bụng chướng: chướng hoi trong ruột
+Bụng báng: có dịch trong ổ bụng
*Một trẻ HCTH biểu hiện đau bụng cấp, có báng bụng/chướng bụng kèm sốt thì nghĩ đến những nguyên nhân gì ?
– Viêm phúc mạc nguyên phát: Sốt, đau bụng, khám có bụng báng, ấn đau khắp bụng => bé này nghĩ nhiều đến dạng này
-Viêm phúc mạc thứ phát: viêm ruột thừa thủng ( Diễn tiến đau thường là ban đầu đau thượng vị, sau đó lan hố chậu phải, sau đó đau khắp bụng)
-Viêm tụy cấp
-Viêm dạ dày ruột
-Viêm loét dạ dày tá tràng (do cort)
-Nhồi máu mạc treo ( do tăng đông trong HCTH)
Bé này khám có bụng báng, ấn đau khắp bụng, nên nghĩ nhiều đến viêm phúc mạc ( các viêm khác thường đau không nhiều hoặc đau khu trú ở vị trí điển hình) => trẻ còn nhỏ nên VPM thường bụng vẫn mềm, ít khi có phản ứng thành bụng, dấu hiệu ấn đau khắp bụng quan trọng, chỉ cần ấn nhẹ cũng đau (đau nhăn mặt, lấy tay gạt tay mình ra) ( người lớn mới có bụng cứng như gỗ, phản ứng phúc mạc)
Phân biệt đau do bụng báng, ấn mạnh thì áp lực ổ bụng tăng => cũng đau nhưng đau không nhiều và lực phải ấn mạnh
4/ Bé này sau khi siêu âm thấy có dịch, làm gì tiếp theo để chẩn đoán VPM và phân biệt nguyên phát hay thứ phát ?
Chọc dịch ổ bụng, đếm tế bào và nuôi cấy
> 100 BC/1mm3 và chủ yếu là đa nhân (VPM do vi trùng) + Cấy ra tác nhân
*Phân biệt nguyên phát – thứ phát : Soi tươi và nhuộm gram
-VPM nguyên phát: => Soi ra/ nhuộm gram ra 1 loại vi khuẩn và là tác nhân hàng đầu gây VPM nguyên phát: Song cầu gram dương hình hạt cà phê (Phế cầu); trực khuẩn gram âm (Ecoli); Cầu khuẩn gram dương dang chuỗi (Liên cầu)
-VPM thứ phát: Thấy cả gram âm và gram dương => thủng tạng rỗng VK chạy trong ống tiêu hóa ra
*VPM Nguyên phát => chỉ điều trị kháng sinh
*VPM Thứ phát => HC ngoại khoa để điều trị nguyên nhân tiên phát
5/ Chẩn đoán bé này
HCTH tái phát không thường xuyên, biến chứng VPM nhiễm khuẩn nguyên phát
6/ Tại sao chọn Cepha3 mà không là KS khác ?
-VPM nhiễm khuẩn nguyên phát: hàng đầu là phế cầu và trực khuẩn đường ruột => Cepha 3 có thể phủ cả gram âm và gram dương
+Sau 48h đánh giá lại lâm sàng, nếu đáp ứng thì dùng cho đủ 7-10 ngày
+Nếu vẫn còn sốt, đau bụng, đừ + KQ cấy máu không mọc. Làm gì tiếp ?
1.Tìm xem còn ở nhiễm trùng khác không ? => Viêm phổi, Viêm da, nhiễm trùng huyết, viêm màng não,
2.Vi khuẩn này không đáp ứng với KS hiện tại => phối hợp 2 KS
.Phế cầu kháng thuốc => Vancomycin
.VK gram âm không đáp ứng => Cefepim hoặc Cirpofloxacin, cuối cùng mới là Carbapenem
*Sau khi đổi KS, Vi sinh báo cấy máu thấy Cầu khuẩn gram dương dạng chuỗi => dùng tiếp KS hay đổi KS ?
=> Tin tưởng do KQ cấy máu ít khi ngoại nhiễm và ra tác nhân phù hợp với tác nhân của VPM, kèm theo lâm sàng bé ổn dần
=> Ngưng carbapenem, giữ vancomycin
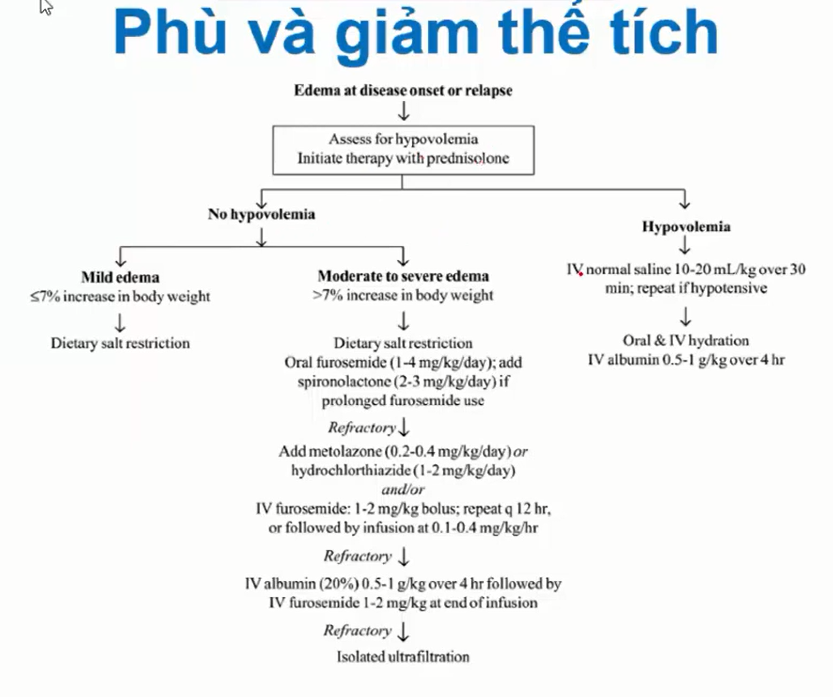
7/ Bé này có cần điều trị giảm phù cho Bn không ?
-Phù dưới 7% trọng lượng cơ thể
-Không khó thở, không ảnh hưởng sinh hoạt hàng ngày
=> không cần giảm phù
=>Khi nào cần điều trị giảm phù
-Tăng > 7 % trọng lượng
-Tràn dịch các màng lượng nhiều: bụng, phổi, tim -> Suy hô hấp
-Di chuyển khó khăn, nằm nhiều sẽ có nguy cơ biến chứng tắc mạch
1.Giảm ăn muối, nước theo nhu cầu
2. Lợi tiểu: Furosemid uông -> chích, có thể kết hợp Furro + Spironolacton (giảm thất thoát kali) hoặc Furo + Thiazide để tăng hiệu quả
3. Truyền Albumin: Albumin 20% liều 0,5-1mg/kg TTMtrong 4 tiếng + Lợi tiểu chích giữa kì truyền ( lúc truyền đc 2 giờ và khi kết thúc truyền) => Lợi tiểu cần protein chuyên chở tới quai henle để có tác dụng, nếu đạm máu thấp quá thì lọi tiểu không đáp ứng
4. Lọc máu ngắt quãng
*Dùng lợi tiểu phải đảm bảo
-không có giảm thể tích nội mạch
-Không có YTNC giảm thể tích nội mạch: ói, tiêu chảy, mạch nhanh, HA hạ
*Truyền Albumin phải chú ý: bệnh nhân phải không có suy thận thực thể
=> Creatinin máu tăng so suy thận tại thận => truyền Albumin vào, kéo dịch vào lòng mạch mà BN không tiểu ra được => quá tải dịch => phù phổi
*Phân biệt suy thận chức năng và suy thận thực thể
8/ Kế hoạch điều trị tiếp theo
-Về nhiễm trùng: nếu đáp ứng lâm sàng tốt, dùng đủ 7-10 ngày rồi ngưng, không cần làm lại bilan nhiễm trùng. Khi nào diễn tiến không thuận lợi, sốt lại hoặc đoạn sau đáp ứng kém dần => làm lại
-Về HCTH
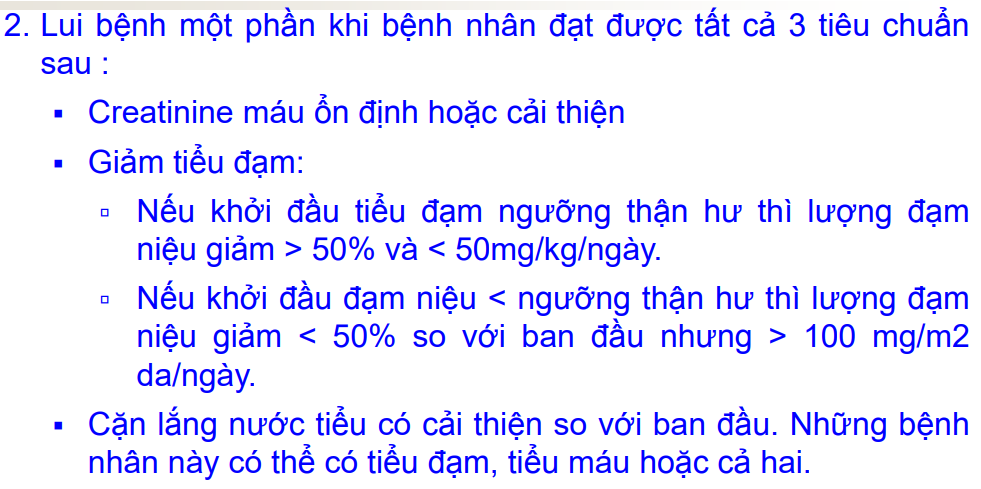
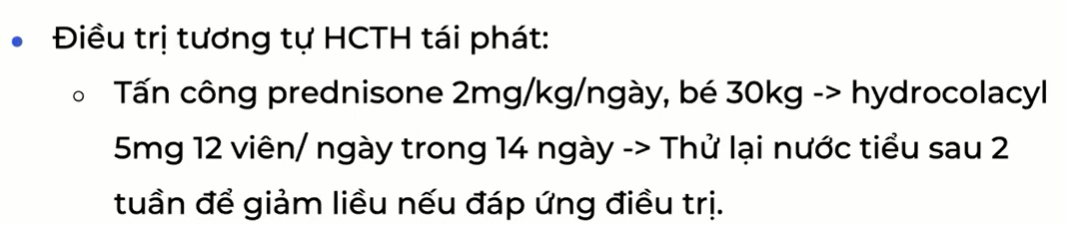
*Nếu sau 14 ngày
– Không đạt lui bệnh:
-Tấn công thêm cho đủ 4 tuần
-Nếu sau 4 tuần vẫn không đạt lui bệnh => tấn công tiếp 2 tuần + thêm Enalapril để giảm đạm niệu ( BN không suy thận hoặc có nguy cơ giảm thể tích tuần hoàn)
-Sau 6 tuần mà vẫn không lui bệnh => HCTH kháng cort muộn
=> Sinh thiết thận + thuốc ức chế Calcineurin=>
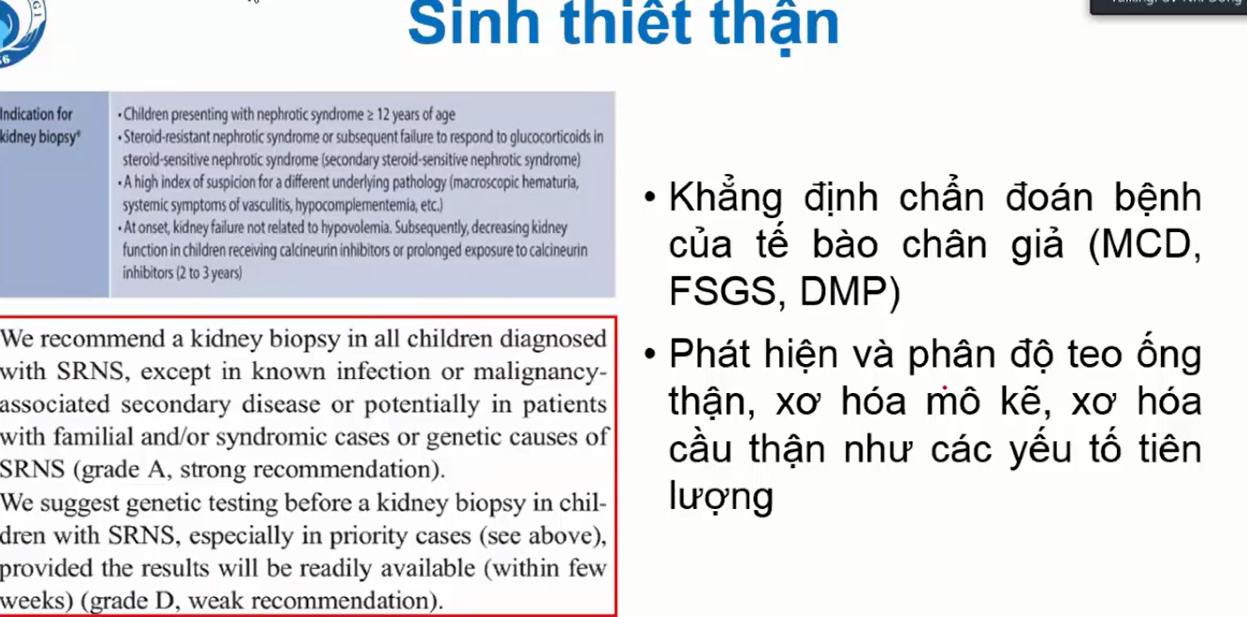
–Sinh thiết thận để
-Khẳng định đây là HCTH nguyên phát: 1 trong 3 dạng sang thương tối thiểu, xơ hóa khu trú từng phần , tăng sinh gian mạch và không có phức hợp miễn dịch
-Xem mức độ tổn thương ống thận mô kẽ => Khi xài Ức chế Calcineurin cần theo dõi sát sợ suy thận. Tiên lượng có nguy cơ diễn tiến tới suy thận mạn không ? => xơ hóa nhiều => tiên lượng xấu
–Thuốc ức chế Calcineurin (Cyclosporin E(BHYT chỉ thanh cho thuốc này), tacrolumux)
=> có nguy cơ độc thận => giai đoạn cấp làm giảm tưới máu thận, tăng creatinin máu thoáng qua
-Điều trị kéo dài trên 2 năm => tổn thương mô kẻ thận không hồi phục (xơ hóa dạng dải băng) => xơ hóa mạch máu thận
=> Theo dõi Kali máu, Crearinin máu
=> Tại thời điểm 2 năm mà vẫn phải dùng thuốc nữa hoặc bất cứ lúc nào thấy creatinin tăng cao => phải nghi ngờ ngộ độc => XN Định lượng nồng độ thuốc (bao nhiêu ?…..), sinh thiết thận tìm dấu hiệu ngộ độc (là gì? …..)
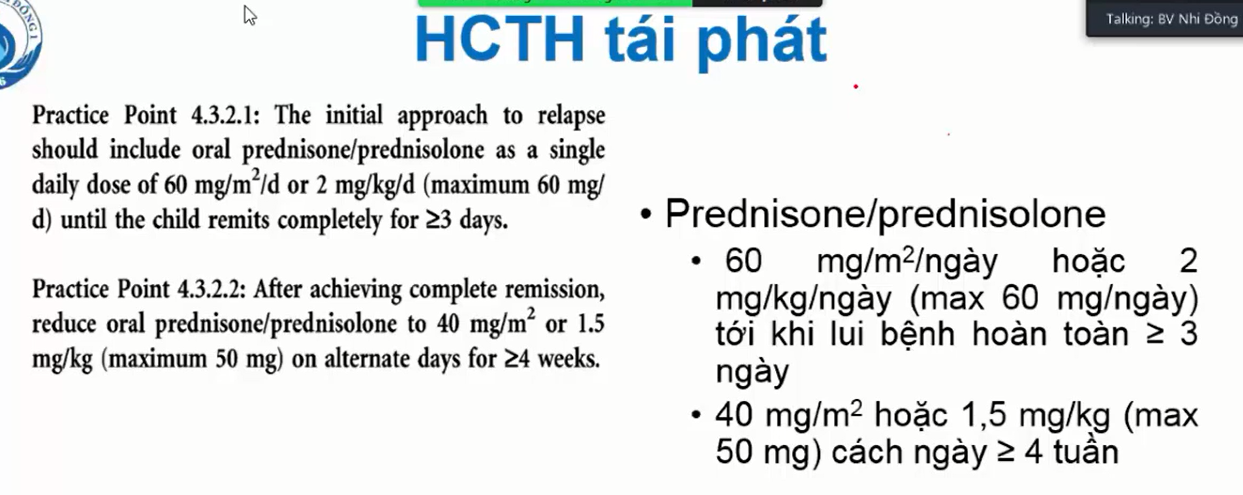
–-Đạt lui bệnh hoàn toàn: hết phù, đạm niệu âm tính 3 ngày liên tục
Đang liều 2mg/kg/ngày -> 4 tuần
-> 1,5 mg/kg/ cách ngày trong -> 4 tuần => sau đó ngưng
Xem hướng dẫn mới KDIGO 2021
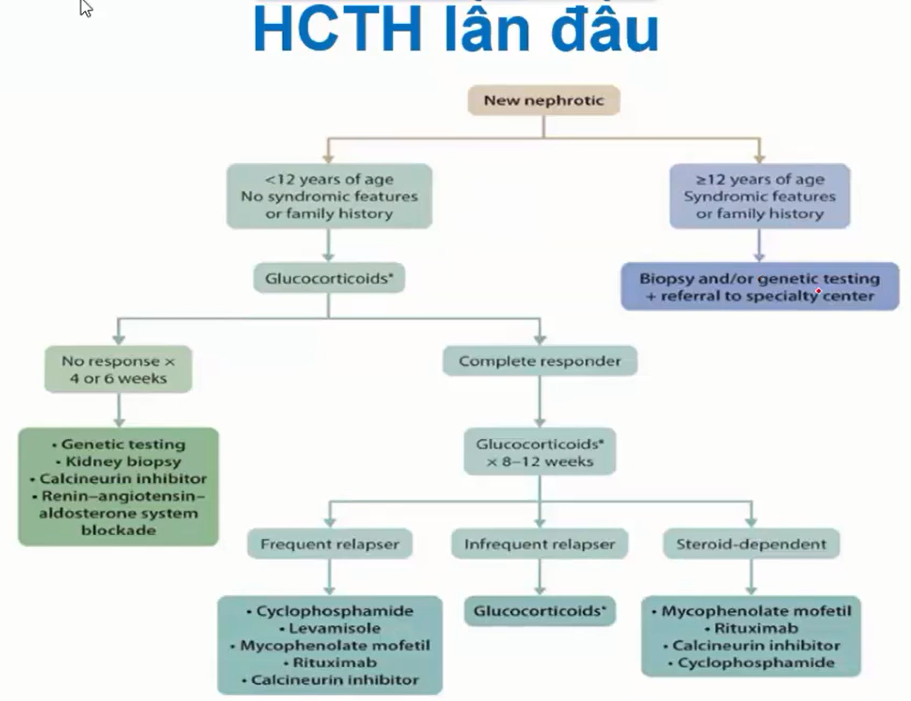
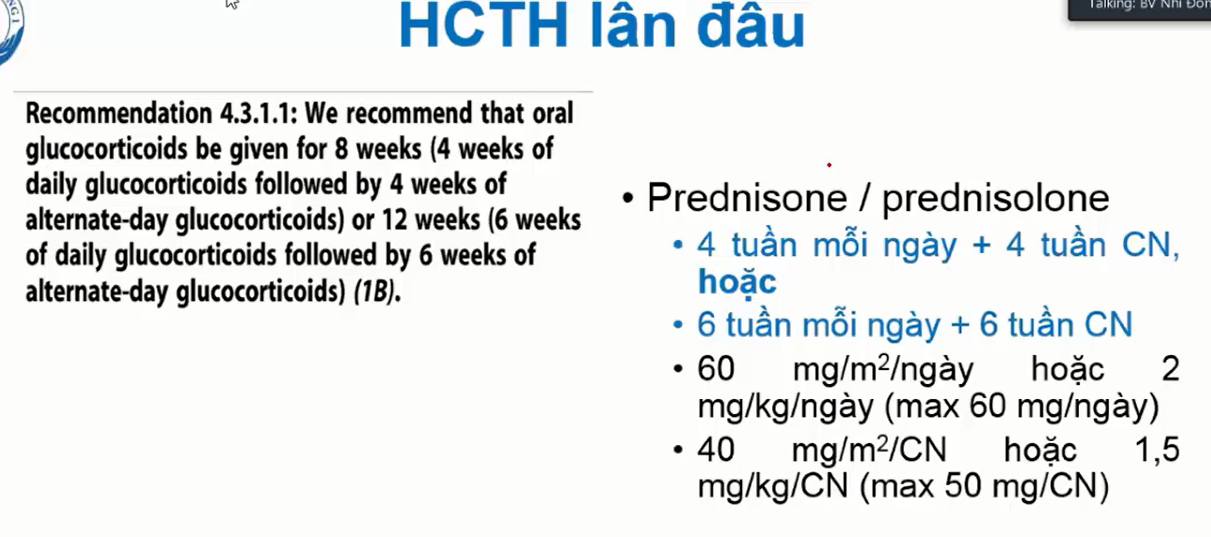
9/ HCTH lần đầu
Phác đồ bệnh viện dùng 4-8-6 => kết thúc sau 3,5 tháng
Xu hương ngày nay dùng 4-4 hoặc 6-6 do: Dùng cort thời gian dài có thể giảm nguy cơ tái phát sau khi đáp ứng hoàn toàn, tuy nhiên, về lâu dài, không giảm nguy cơ lệ thuộc hoặc tái phát thường xuyên
*Khi nào chọn tấn công 4-4
-Trẻ đạt lui bệnh sớm trong 7 ngày
-Có các bệnh đồng mắc làm tăng nguy cơ bị tác dụng phụ của cort: Béo phì, THA, DTD type 1
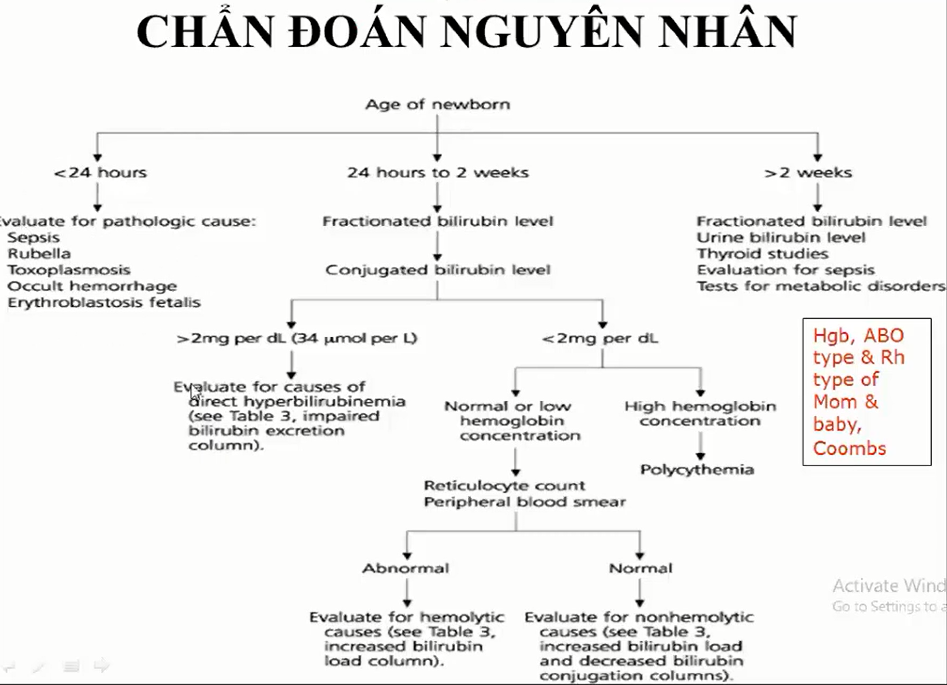
1/ Dựa vào đâu chẩn đoán lâm sàng là vàng da tăng Bilirubin GT
1.Thời điểm xuất hiện
2.Màu săc da
-Vàng chanh -> tăng Bili trực tiếp
-Vàng cam -> Tăng Bili gián tiếp
3.Nước tiểu + Phân
– Nước tiểu sậm + phân bạc màu => Bili trực tiếp
– Nước tiểu vàng trong + phân vàng => Bili gián tiếp
2/ Biện luận chẩn đoán
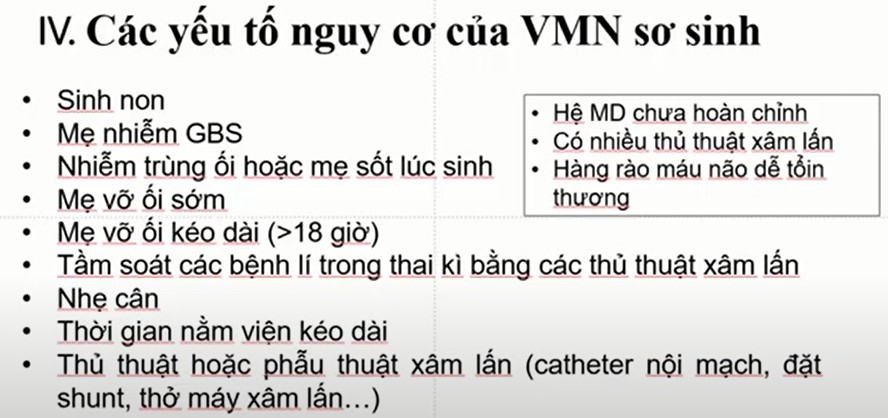
-Trẻ có dấu hiệu nhiễm trùng huyết => cần chẩn đoán phân biệt VMN do tác nhân dễ đi qua hàng rào máu não vào khoang màng não
– Nghi ngờ có bất thường đường tiêu hóa đi kèm : Ọc dịch vàng xanh, bụng chướng, không rõ tiêu phân su (Tắc ruột, ruột xoay bất toàn…)
=> Bé sanh non, có dấu hiệu không dung nạp đường tiêu hóa => dùng từ viêm ruột hoại tử phù hợp hơn Chẩn đoán viêm ruột
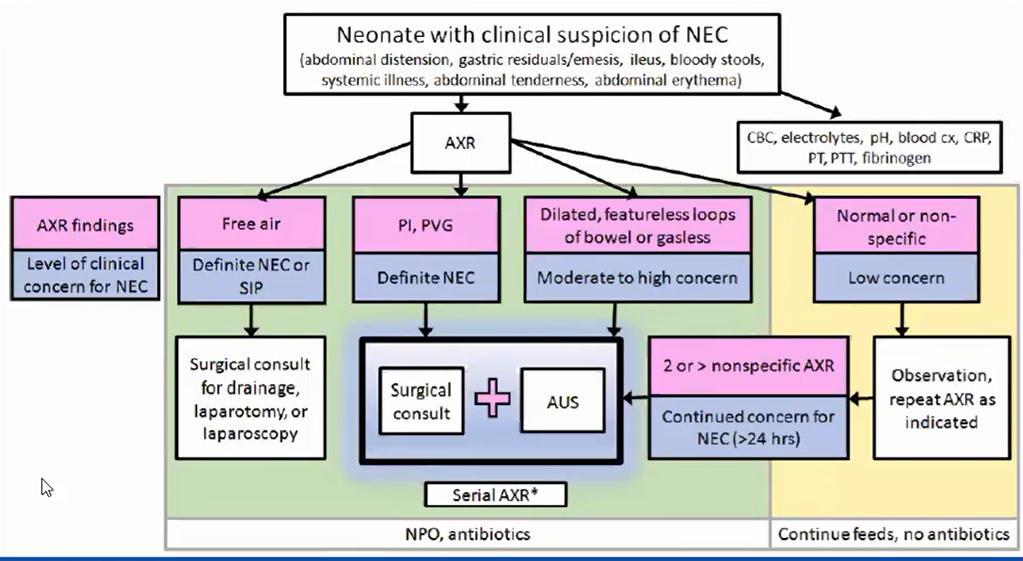
3/ Đề nghị CLS phải đạt được mục tiêu chẩn đoán chưa ?
-Vàng da
-Viêm ruột hoại tử
-Nhiễm trùng
-Viêm màng não
4/ Bé vàng da có chỉ định chiếu đèn chưa ?
So sánh bảng chỉ định chiếu đèn
Trẻ đủ tháng: ngưỡng chiếu đèn = 5 x P(kg)
Trẻ non tháng: là 1 yếu tố nguy cơ vàng da nặng => ngưỡng chiếu đèn thấp hơn trẻ đủ tháng
5/Bé này tại sao dùng Cipro mà không tiếp tục Cefo/Genta tiếp ?
Đã điều trị trước đó ở BV trước bằng Cefo/Genta, chuyển viện, nhưng tình trạng nhiễm trùng hiện tại nặng nề hơn, xuất hiện triệu chứng nhiễm khuẩn mới => hướng nghĩ đến nhiễm trùng sơ sinh muộn, có thể là tác nhân bệnh viện => nâng lên Cipro
-Nếu bé đã điều trị ở BV cefo/genta, sau đó khỏe, về nhà được 1 thời gian rồi nhiễm trùng lại => xem như nhiễm trùng mới từ cộng đồng, có thể dùng lại cefo/genta
6/ Tiêu chuẩn
-Nhiễm trùng bệnh viện
-Nhiễm khuẩn cộng đồng
7/ Tìm nguyên nhân gây vàng da ?
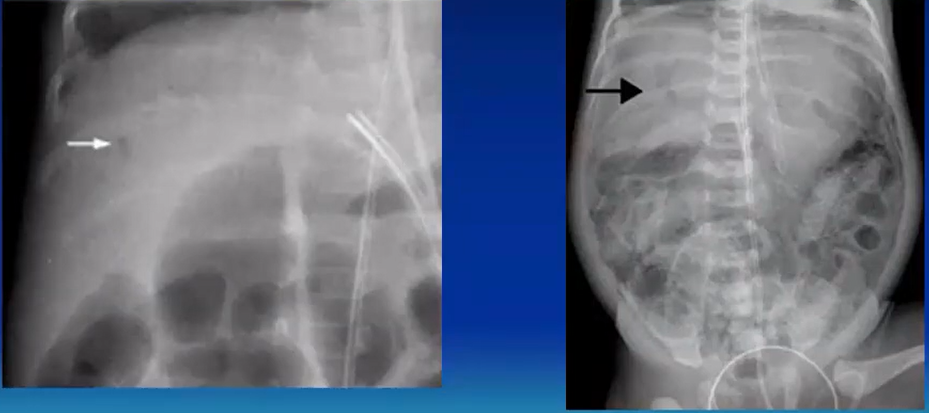
8/ Xquang bụng
-Chất lượng phim: tương phản rõ giữa khí và mô. Tia cứng: hình ảnh tổn thương bị giảm đi, tia mềm thì nhìn bị mờ
-Tư thế
-Hình ảnh:
+Quai ruột dãn
+Hơi trong thành ruột không ?
+Có dịch trong ổ bụng không ?
+Thành ruột có dày không ?
+Có hơi trong tĩnh mạch cửa không ?
+Có khí tự do trong khoang bụng không ? => thủng ruột
9/ Sonde dạ dày ghi ra ít dịch trắng – xanh ?
Không ghi vậy
Xanh đậm – nhạt – xanh rêu
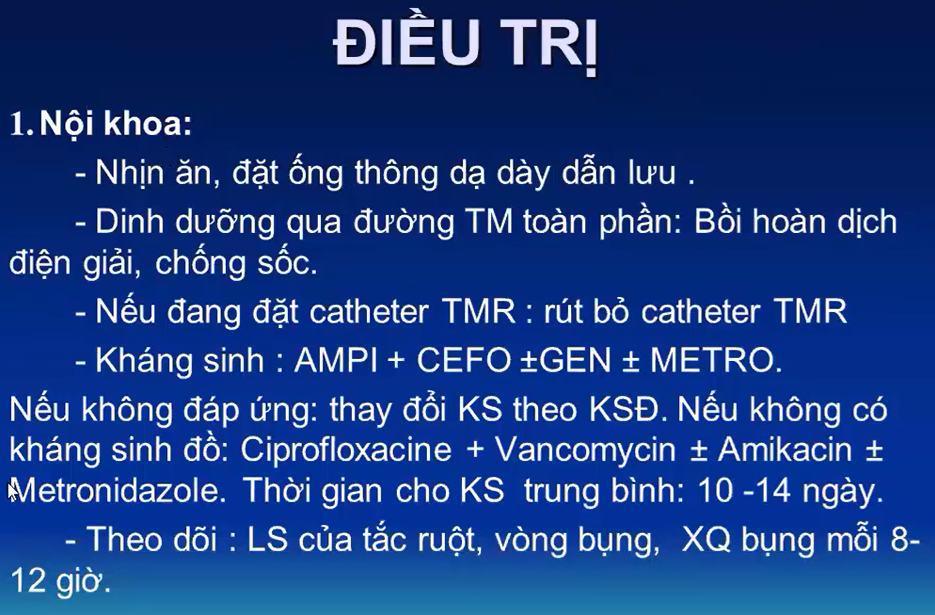
10/Kháng sinh
Tại sao Meropenem điều trị được gram âm kị khí mà vẫn thêm Metronidazole ?
Mero là kháng sinh phổ rộng, hướng về điều trị gram âm là chủ yếu, không thiên về Vk kị khí. Metro tập trung điều trị kị khí => phối hợp trong Viêm Ruột Hoại Tử ở trẻ sơ sinh
Khi nào quyết định dùng Metronidazole ? => Có hơi thành ruột hoặc nghi ngờ có biến chứng của VRHT
*Trong phác đồ, nếu không đáp ứng Ampi + Cefo thì chuyển sang Meropenem + vanco => sao bé này không dùng
-Có nguy cơ nhiễm trùng gam dương: Catheter TM
-Nhiễm trùng nặng
-Cấy máu ra vi khuẩn nhạy Vanco
11/ Tại sai tăng sữa từ từ mà không tăng nhanh ?
Trong trường hợp không có sữa mẹ thì thay thế bằng sữa gì ?
12/
13/
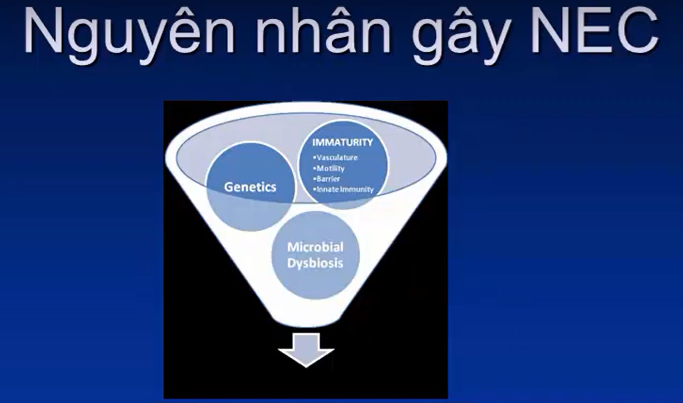
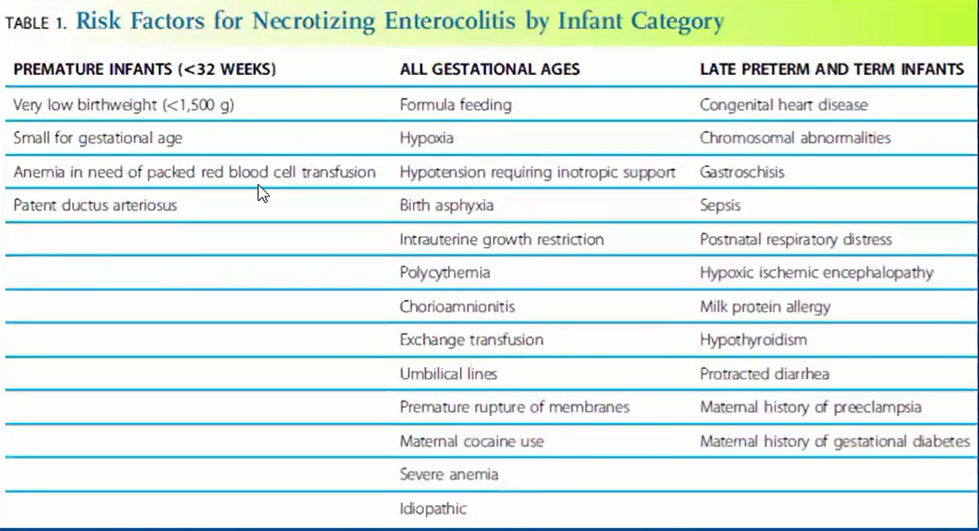
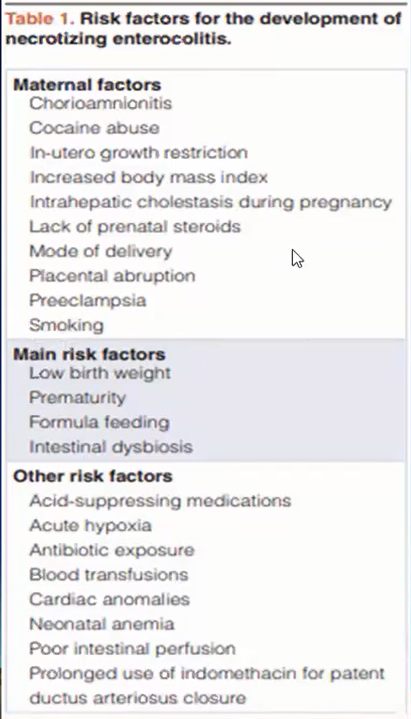
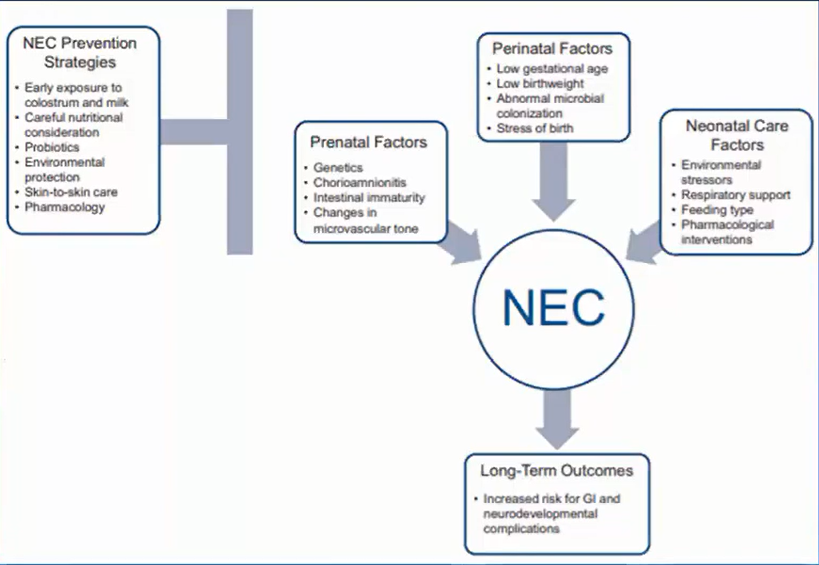
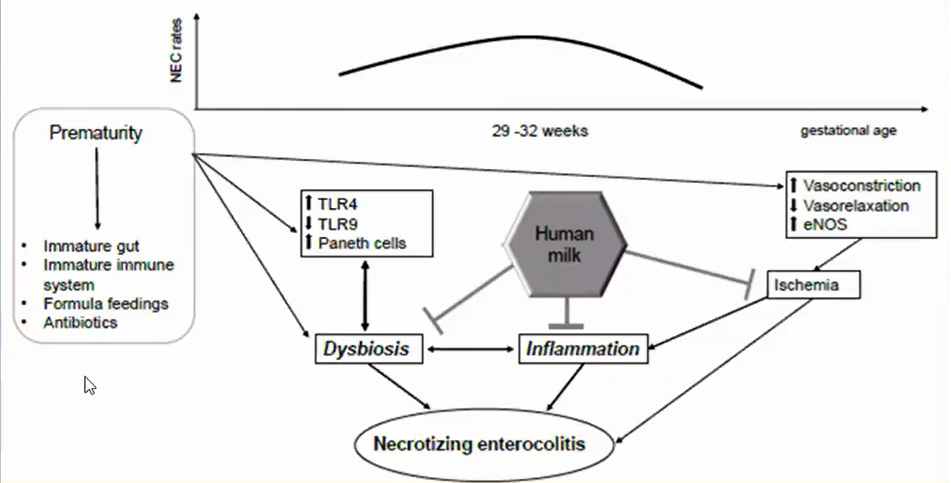
14/ RF Viêm ruột hoại tử
-Đa hông cầu (Hct >65%) => máu bơm đi chậm => giảm tưới máu tới ruột
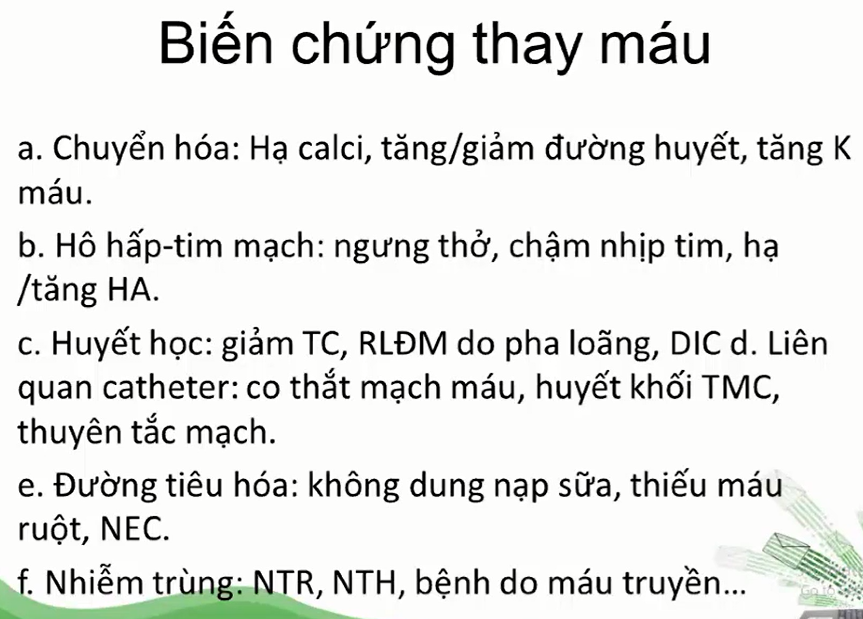
-Thay máu => phải cho nhịn trước và 6h sau khi thay máu => do thay máu làm thay đổi huyết động máu => ảnh hưởng máu đến ĐM mạc treo tràng trên => tưới máu ruột
-Đối với trẻ sanh non: nhóm cho tăng sữa 10-20ml/kg/ngày so với 30-40ml/kg/ngày không có sự khác biệt về giảm nguy cơ viêm ruột hoại tử. Tuy nhiên đây chỉ là bé sanh non không yếu tố nguy, còn đây là bé đang nhiễm trùng, đang viêm ruột hoại tử => đường ruột có tổn thương, nên tốc độ tăng 10-20ml/kg/ngày an toàn hơn
*Yếu tố nguy cơ độc lập của VRHT (chỉ cần có yếu tố này, không cần kết hợp yếu tố nào khác cũng tăng nguy cơ VRHT)
-Sanh non
-Nhẹ cân
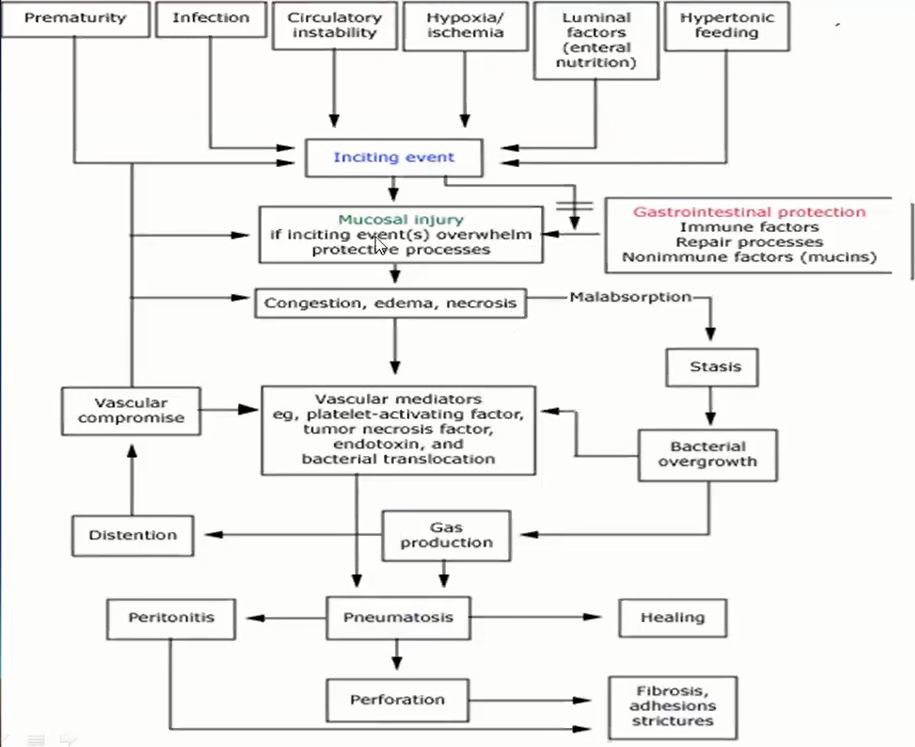
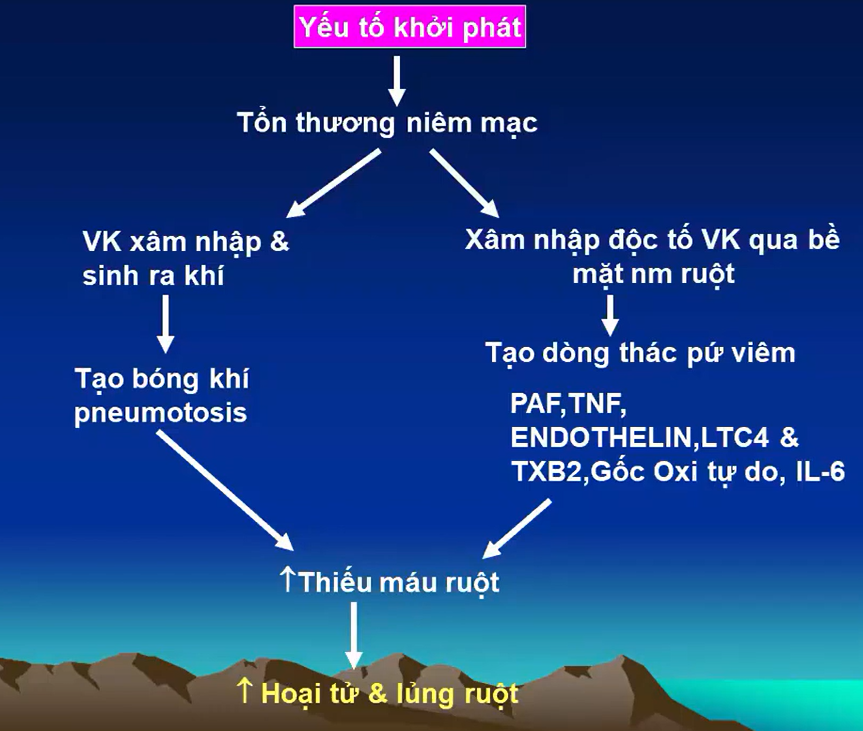
15/ Cơ chế
16/ Trẻ sanh non, nhẹ cân nếu không có bệnh lý nào khác, không có chống chỉ định nên cho ăn sớm => đạt được dinh dưỡng toàn phần đường tiêu hóa và giảm thời gian nằm viện
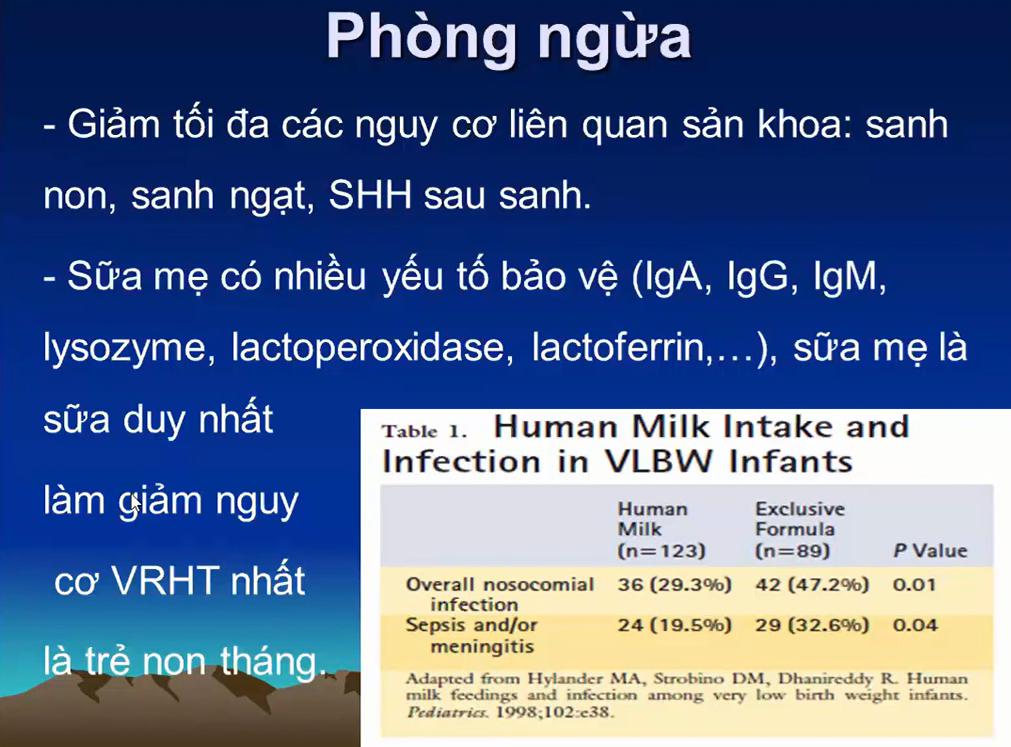
-Sữa non của mẹ: giảm
-Nguy cơ nhiễm trùng
-VRHT
-Sớm đạt được dinh dưỡng toàn phần qua đường tiêu hóa
-Giảm thời gian nằm viện
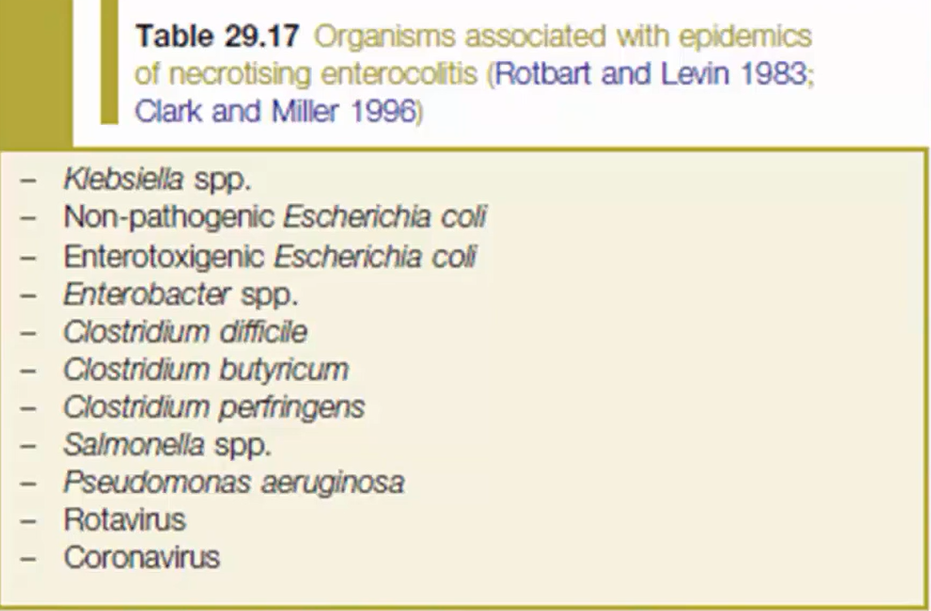
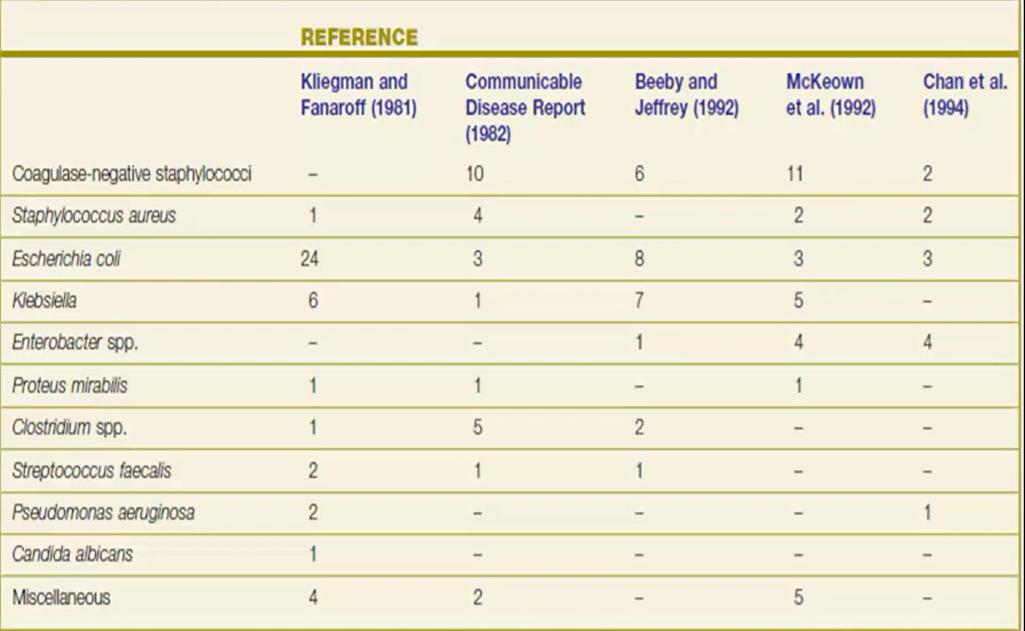
17/ Tác nhân
Riêng ở khoa, các trường hợp VRHT => cấy không ra
17/ Quá trình
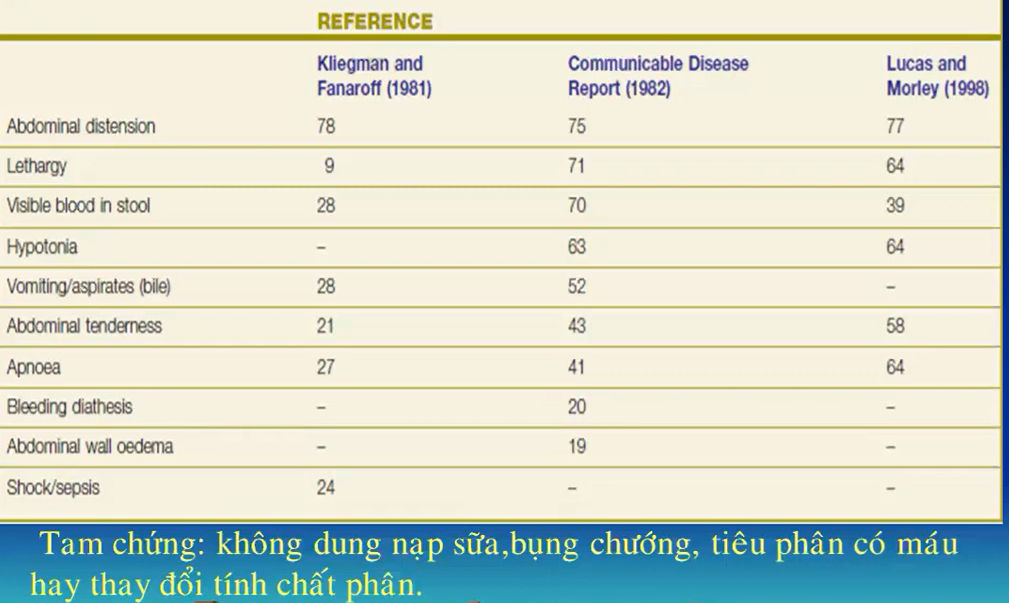
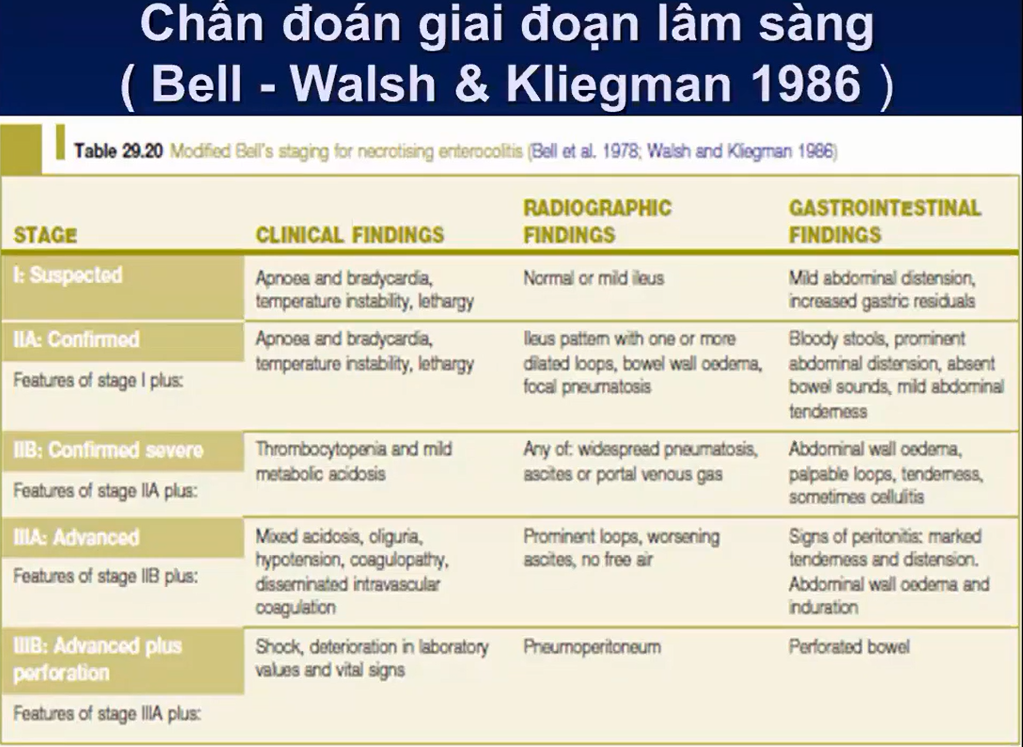
18/ Triệu chứng kinh điển
-Không dung nạp được sữa
-Bụng chướng
-Đi cầu thay đổi tính chất phân: phân nhầy máu, có máu ẩn trong phân
=> Bụng căng chướng + da thành bụng đỏ => coi chừng có viêm phúc mạc
Xquang:
-Hơi vùng gan ( Hơi đi vafoo TM cửa)
-Hơi ở thành ruột
Hình bên (P) => hơi trong tĩnh mạch cửa
-Thường hơi trong TM cửa phải đi kèm hơi trong thành ruột hoặc dày thành ruột
Nếu chỉ là hơi TM cửa đơn lẻ, cần truy lại tiền căn có từng đặt catheter TM rốn chưa ? có thể là hơi do lúc đặt catheter TM đưa vào
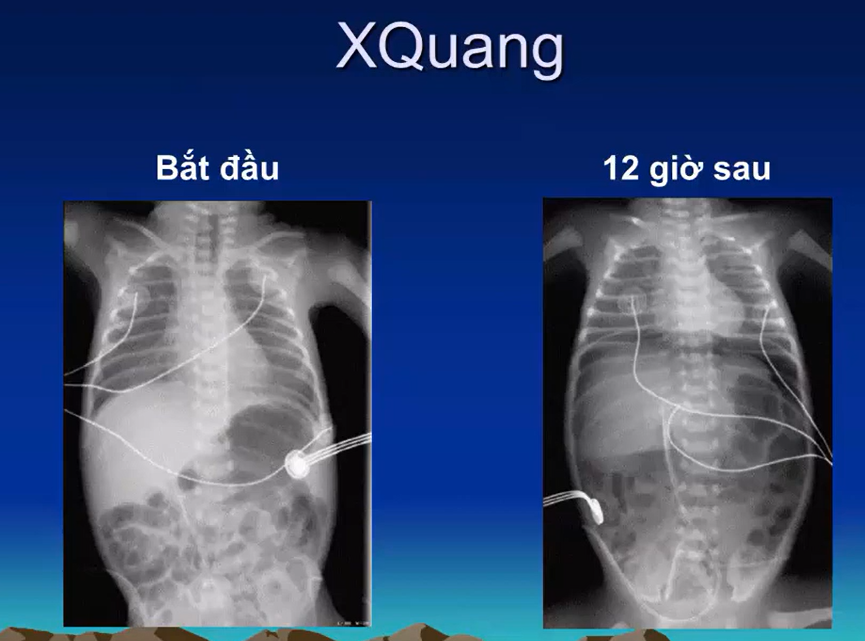
Hình ảnh hơi trong thành ruột ngoài thực thể
Hình 12 giờ sau: thủng ruột, liềm hơi tách gan và cơ hoành ra
Hình ảnh thủng ruột
1/ Hơi len lỏi vào vùng gan, len nào cơ hoành
2/ Hình ảnh tam giác hơi giữa các quai ruột
Thủng ruột
-Bên (T): liềm hơi dưới hoanhf
-Bên (P): Football sign
18/CLS
Triệu chứng kèm theo => Y như nhiễm trùng huyết + chướng bụng + tiêu máu (đại thể, vi thể)
Diễn tiến tới VPM có thể rất nhanh trong vài giờ hoặc kéo dài vài ngày
19/
20/ Điều trị
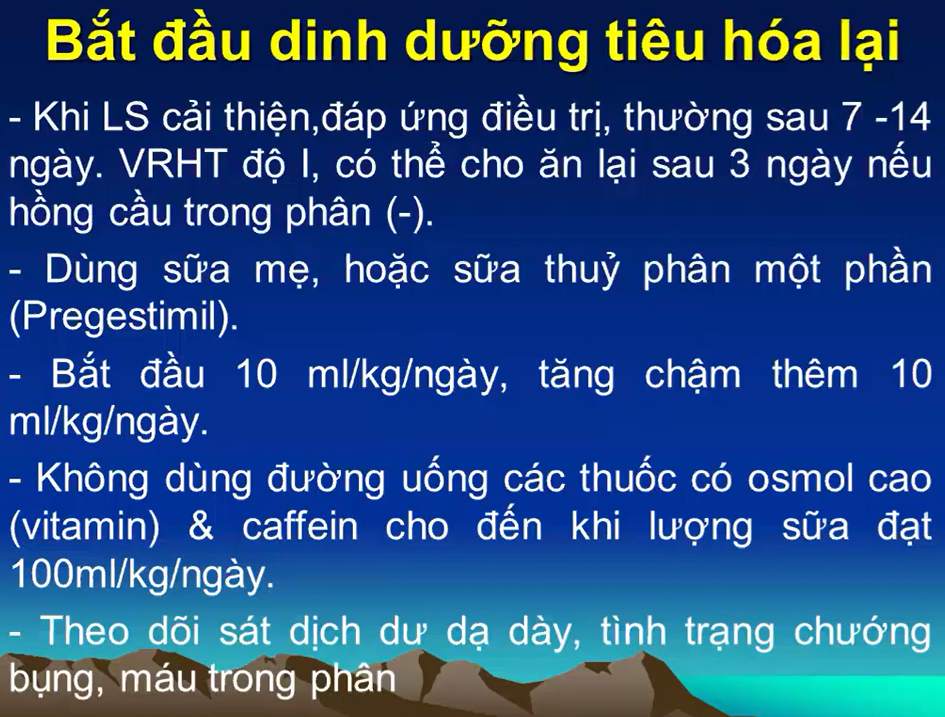
21/ Khi nào cho ăn lại
Dùng sữa thủy phân khi
-Nghi dị ứng đạm sữa bò
-NEC tái phát
-Không có nguy cơ nào khác
22/ Tiên lượng
-HC ruột ngắn
-Tắc ruột do dính
-Nguy cơ ảnh hưởng tới phát triển tâm thần vận động
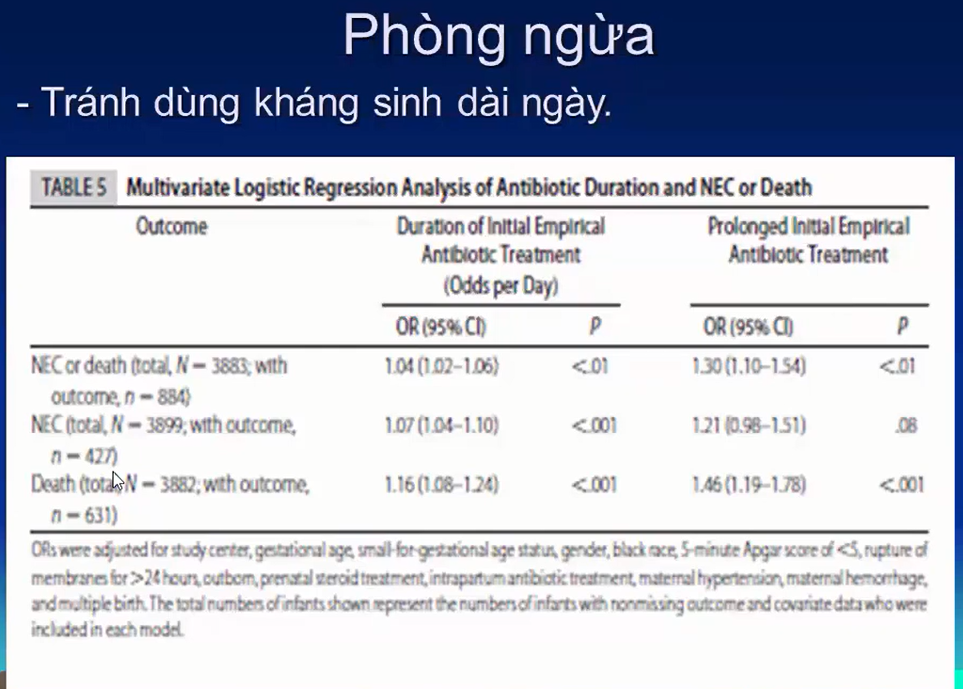
23/Phòng ngừa
23/ Khi nào cho ăn lại
5-7 ngày, nặng thì 7-15 ngày
-Lâm sàng không còn
+Chướng bụng
+Tiêu phân có máu
-Siêu âm (đặc biệt là trẻ có tổn thương thành ruột: hơi thành ruột, hơi TM cửa)
+ Thành ruột dày trên Xquang: 2 thành ruột cộng lại >= 4mm
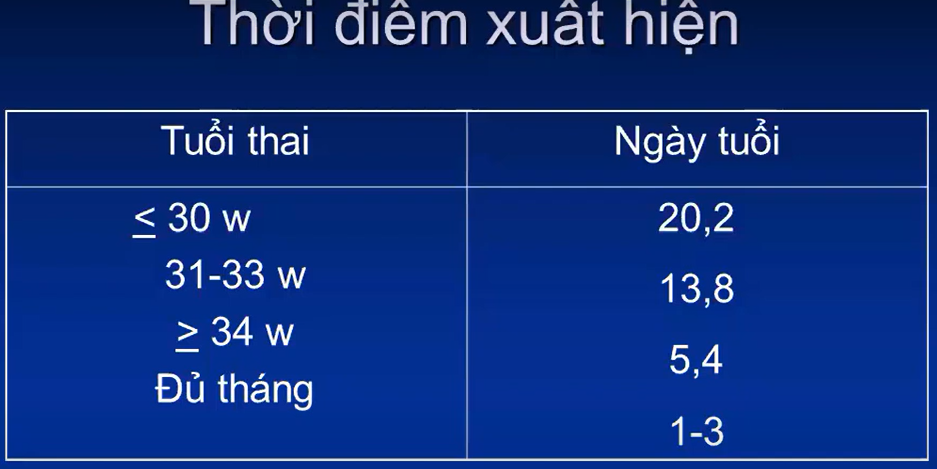
-Dấu hiệu gợi ý tìm nguyên nhân: Thời điểm xuất hiện
-Triệu chứng khác kèm theo (tổn thương não, bướu huyết thanh…)
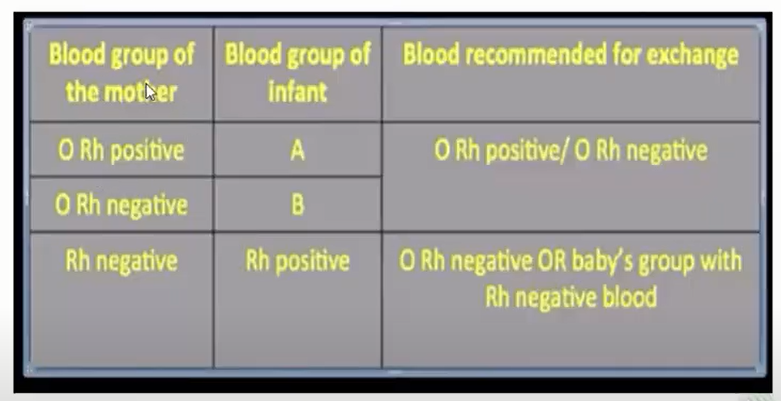
4/Thay máu cần chú ý có chống chỉ định không ?
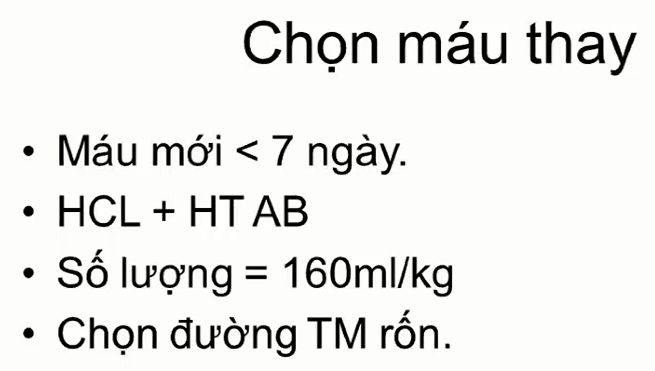
5/ Thay máu: Mỗi chu kì thay
5% thể tích tuần hoàn = 4ml/kg => rút 50% HT tươi đông lạnh – 50% Hồng cầu lắng
6/ Xem xét có cần truyền IvIg không ? => chỉ định truyền khi Bili GT vẫn dưới ngưỡng thay máu 2-3mg/dL dù đã chiếu đèn tích cực => IvIg gắn vào thụ thể Fc của kháng thể => Chỉ dùng khi chưa tới ngưỡng thay máu => vừa chiếu đèn, vừa IvIg để Bili giảm => mục đích là giảm nguy cơ thay máu, Không thay thế cho thay máu
7/Sau thay máu thời điểm nào làm Bili kiểm tra ? => sau thay máu 30p – 1h
Không được lấy máu ở chu kì cuối cùng để làm Xn do lẫn máu mới từ túi máu vào => sai kết quả
8/
9/Có dùng kháng sinh không ?
-Không có YTNC nhiễm trùng sơ sơ: SHH, Sinh khó, mẹ NT….
-Tổng trạng tốt: lừ đừ, sốt, bú giảm, bú kém…
=> không cần dùng KS
Ngược lại, =>. Cho KS ban đầu. Sau đó đánh giá lại LS + CLS, nếu không còn bằng chứng nào của NTSS => 24-48h ngừng KS
10/
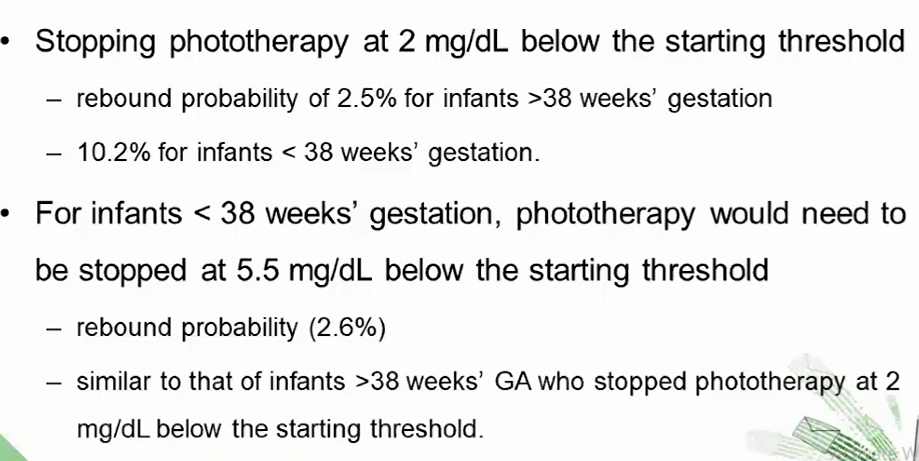
11/Hiện tường Rebound (tăng Bili trở lại sau chiếu đèn)
-Trẻ >38w, ngưng chiếu khi Bili dưới ngưỡng chiếu 2-3mg/dL
-Trẻ <38w, ngưng chiếu chi Bili dưới ngưỡng chiếu 5,5 mg/dL
12/ Thay máu
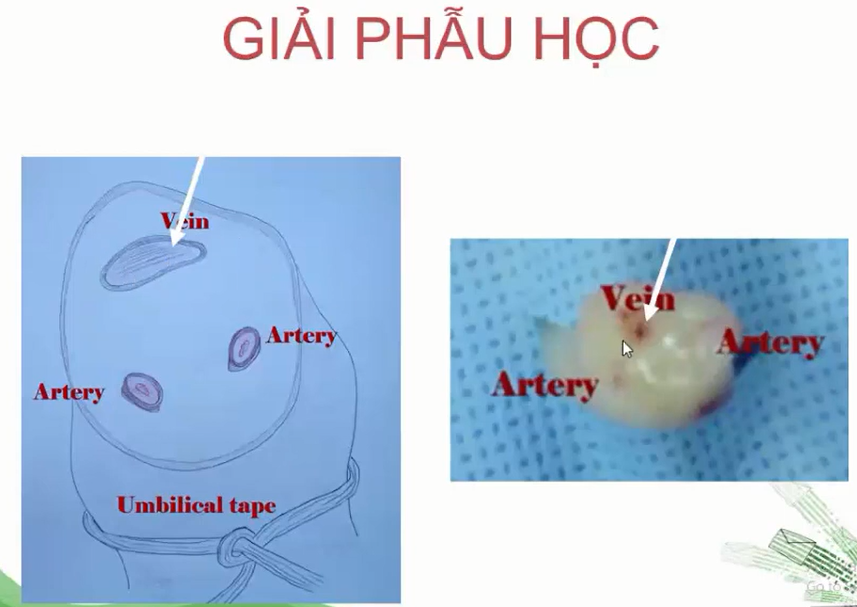
14/Xác định TM rốn
Thường TM rốn nằm ở hướng 11-12h
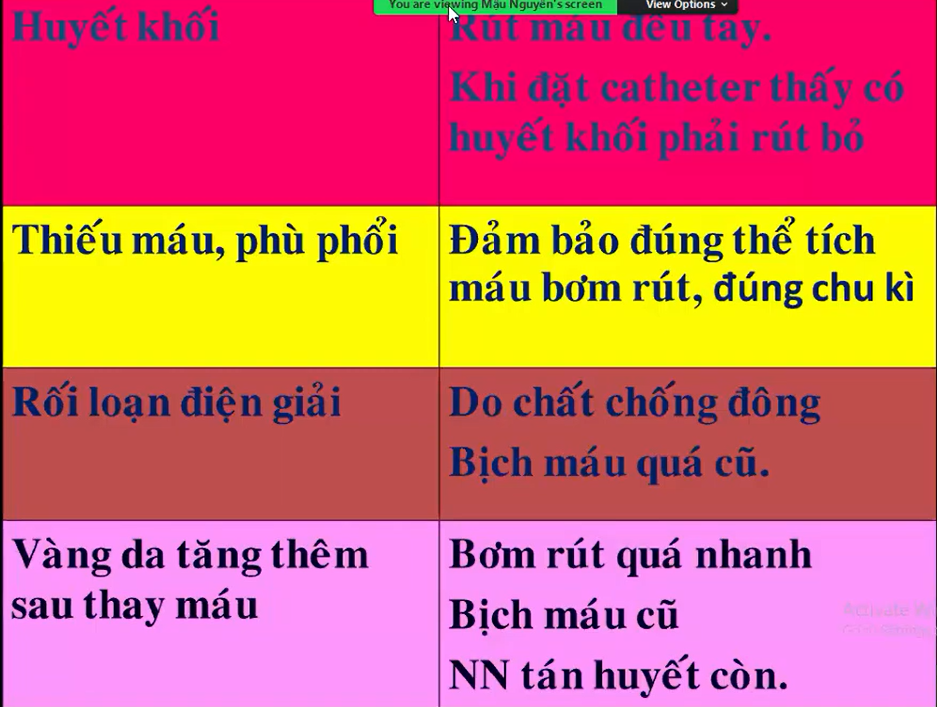
15/ Biến chứng thay máu
TC trong túi máu dự trữ có thể tiểu cầu sẽ hơi thấp do dự trữ lâu, tiểu cầu chết
-Trước thay máu vài tiếng, sau thay máu 6h => tạm nhịn để cho ruột nghỉ ngơi 🡺 giảm nguy cơ biến chứng viêm ruột hoại tử
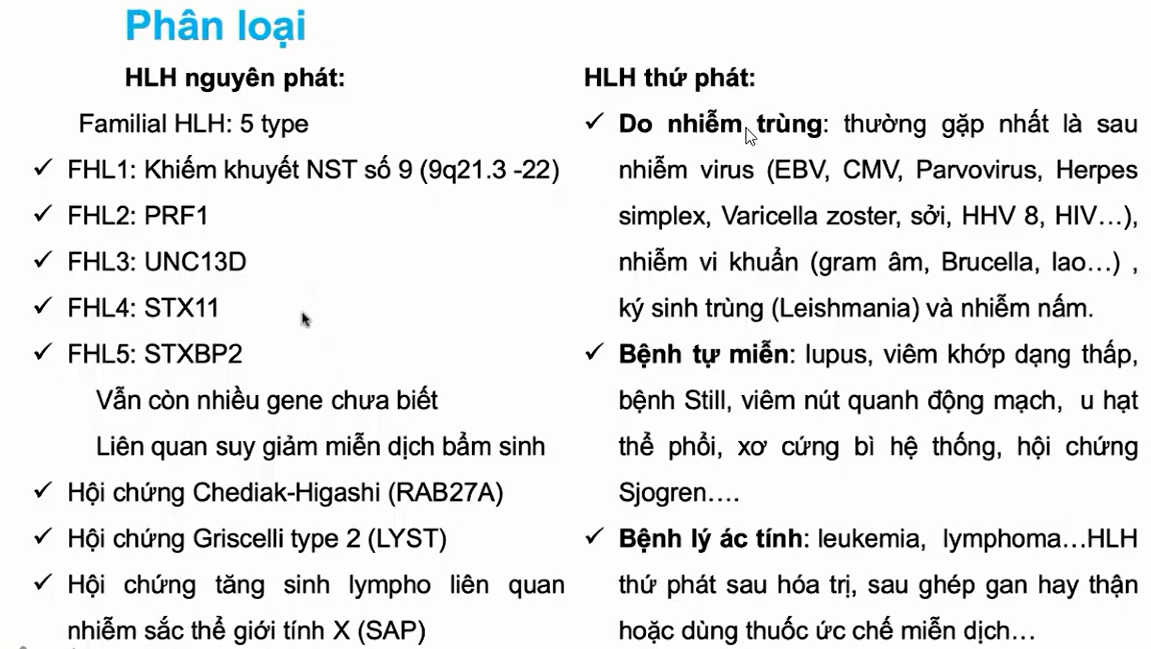
Tác nhân có thể là vi khuẩn (60%), virus , bệnh lý tự miễn, ung thư
=> Ở châu A 60% là do nhiễm trùng => Nếu chưa có gợi ý gì về nguyên nhân, đánh kháng sinh theo kinh nghiệm mạnh, phổ rộng từ đầu, sau đó xuống thang chứ không dùng KS tăng bậc như điều trị bình thường => 24h sau làm lại bilan thực bào
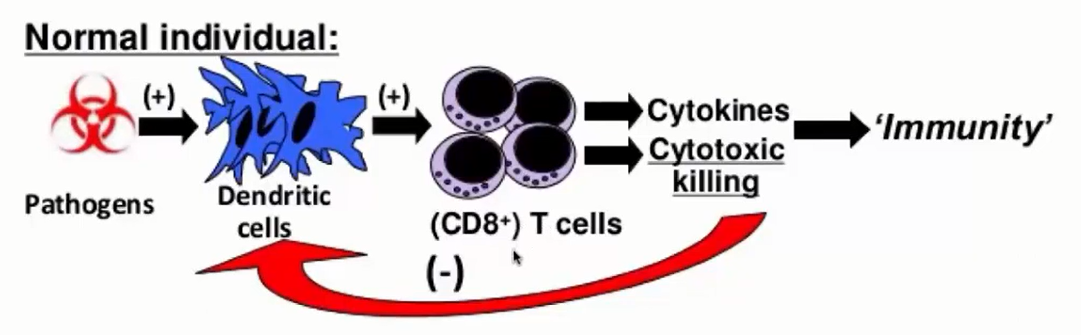
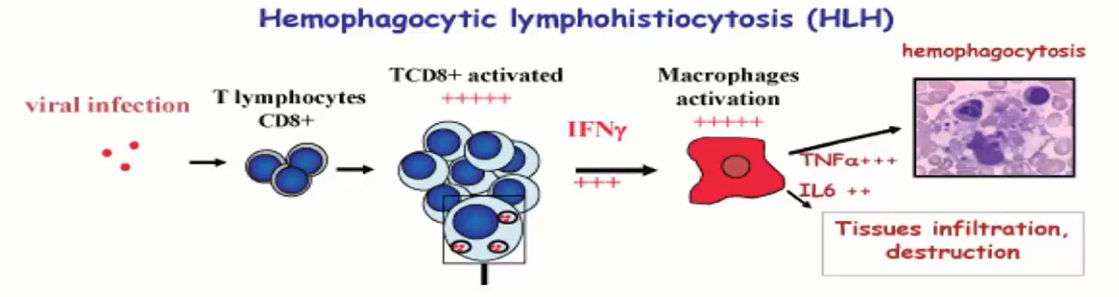
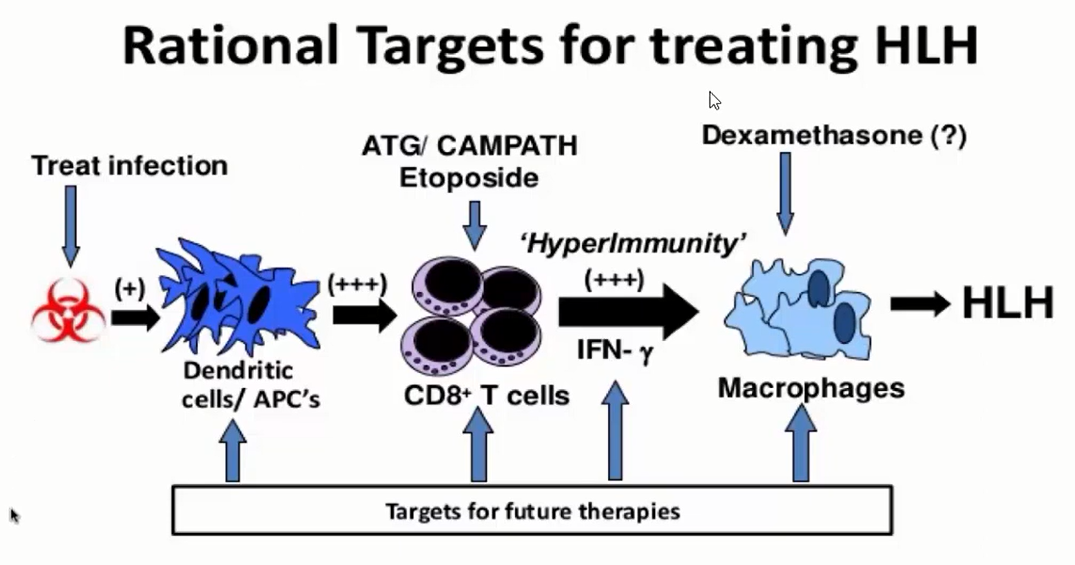
-TB Lympho T có dấu ấn chung là CD3 => trên CD3 có dấu ấn riêng
+Lympho T độc tế bào: CD8 => Bình thường Lympho T CD8 cũng chứa các hạt độc bên trong, khi được kích hoạt lên, giải phóng các hạt độc ra ngoài khỏi Lympho T CD8 => Lympho T Killer
+ Lympho T Helper: CD4
+ NK : dấu ấn CD5,6
*Cytokin quan trọng nhất cần quan tâm là
INF-Gamma (Gamma Interferon)
Hoạt hóa Macrophages
Quá trình chuyển thành fibrinogen: Prothrombin complex -> Fibrinogen. INF-Gamma tăng gây ảnh hưởng đến Prothrombin Complex => Giảm Fibrinogen
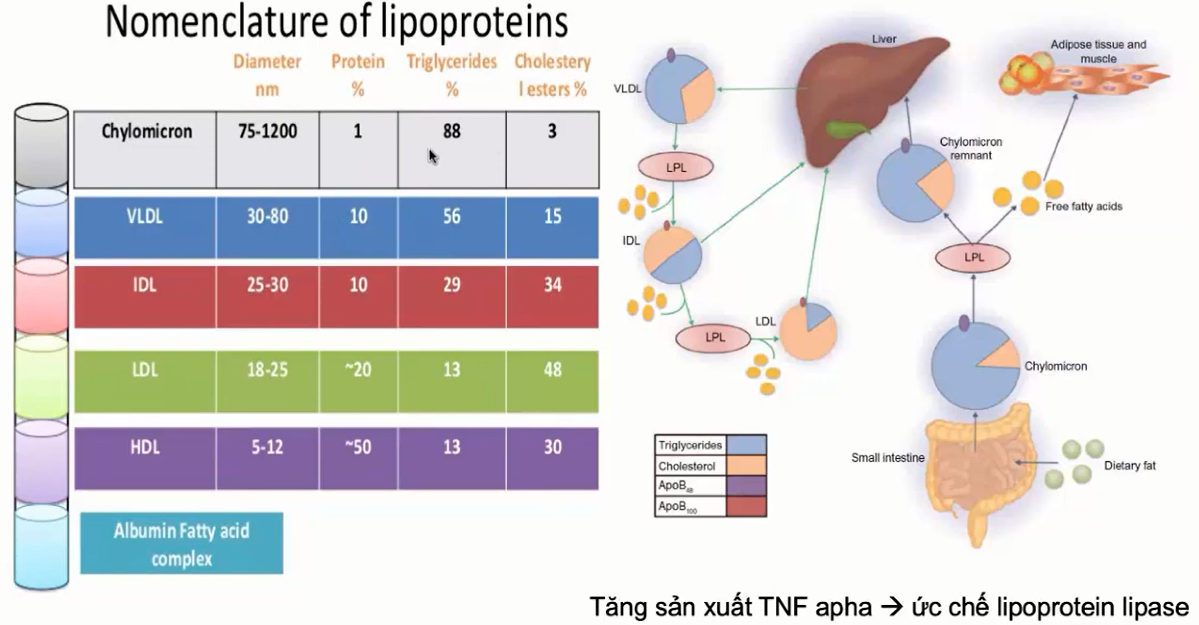
TNF-alpha :
Tăng sinh lượng lớn, làm Macrophages tấn công các TB trong tủy => giảm các dòng TB máu
Ức chế LPL => không thủy phân được Chylomicron => triglycerite tăng
IL6 => Gây tổn thương mô (gan, não…) => tổn thương không hồi phục => tăng men gan rất cao
*Tại sao lại tăng Triglycerite ?
Quá trình thùy phân từ Chylomicron (chứa nhiều triglycerite nhất) -> HDL cần men LPL (Lipoprotein Lipase)
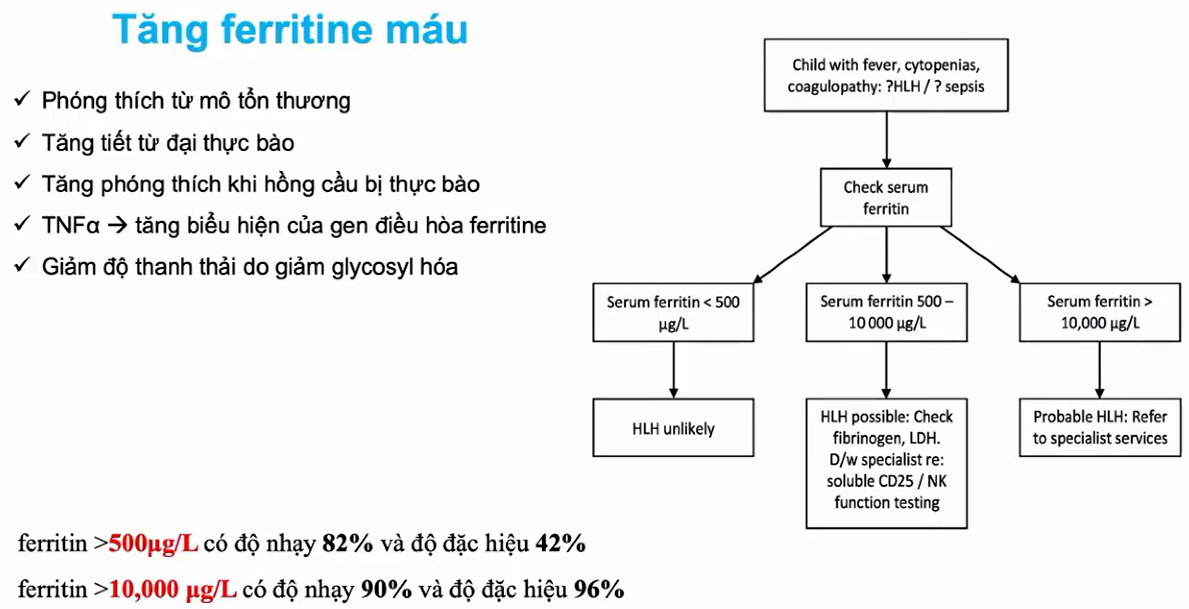
*Tại sao tăng Ferritin ?
Ferritin là 1 protein do gan tạo ra, không phản ánh thật sự sắt dự trữ trong gan, nó chỉ là nơi sắt dự trữ trú ẩn => có hiện tượng tăng giả trong viêm
Nguyên lý chung: khi cơ thể có hiện tượng viêm, hầu hết các protein trong cơ thể đều tăng sản xuất => bao gồm cả ferritin
Mốc 10000mcg/L => chỉ điểm bão Cytokin
*Tổn thương gan trong HC Thực bào có gì đặc biệt ?
Tổn thương Do Cytokin chủ yếu là ty thể => AST tăng cao >> ALT (giống sốt xuất huyết ???)
Khác với Tổn thương gan trong Viêm gan, …
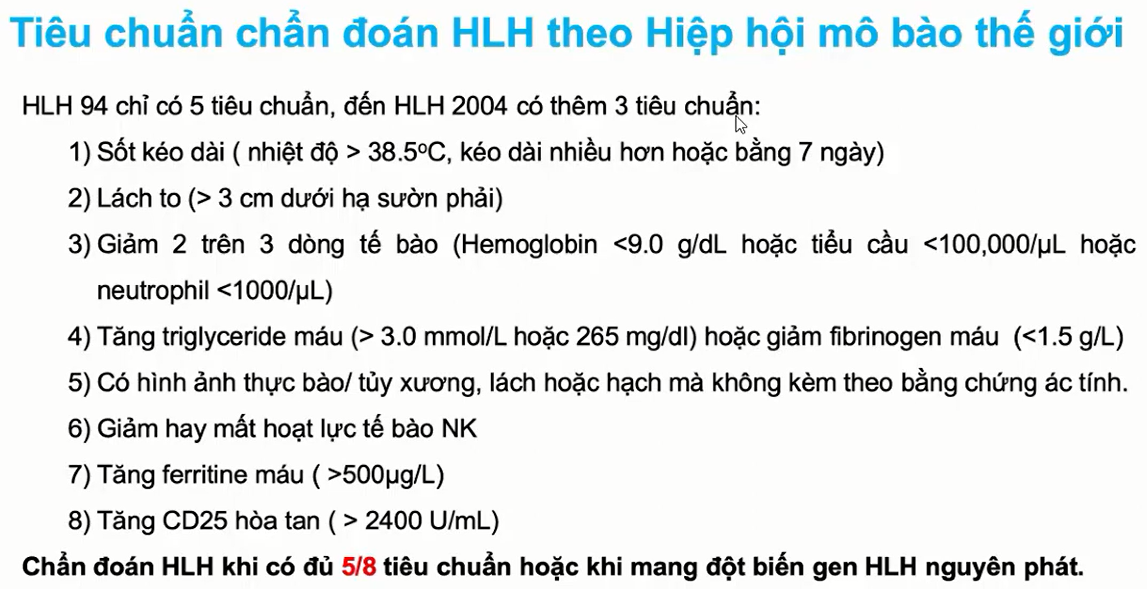
3/ Tiêu chuẩn chẩn đoán
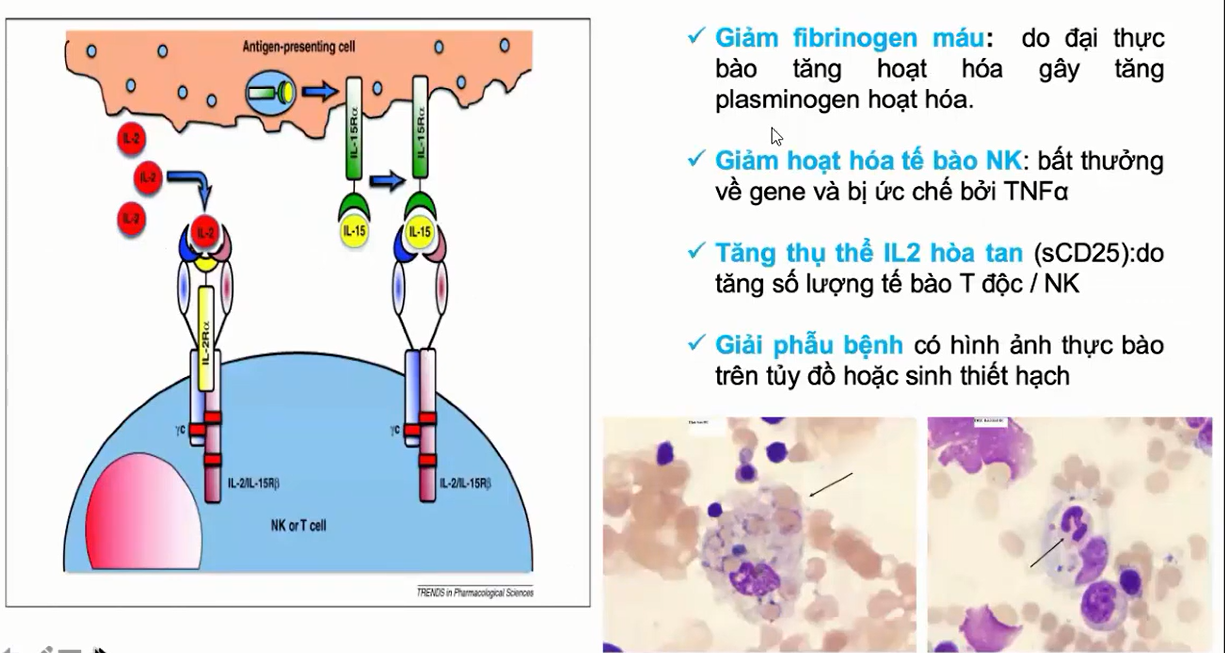
Tiêu chuẩn vàng: Sinh thiết tủy hoặc hạch => thấy hình ảnh Macrophages đang ăn tế bào máu
Không ứng dụng nhiều trên lâm sàng
*Cận lâm sàng thường làm thên LDH => LDH tăng đồng bộ với Ferritin và Triglycerite => ủng hộ việc TB ở mô hoặc cơ quan bị tổn thương vỡ ra, giải phòng LDH
Thực bào là phải có sốt, nếu BN hết sốt 24h rồi thì tạm gác thực bào qua 1 bên. Có thể CLS sẽ đi sau lâm sàng (2-3 ngày sau sẽ hồi phục), tuy nhiên, thực bào là phải có sốt
4/ HC thực bào đã vào Bão Cytokin chưa ?
=> Đủ 4 tiêu chuẩn
1.Ferritin > 10.000 mcg/L
2. Triglycerite > 7 mmol/L
3. LDH > 3000
4. Kèm theo 3 dòng giảm rất sâu
Nếu chỉ có Ferritin tăng đơn độc, nên tìm nguyên nhân
Tự Miễn
RL Miễn dịch
Bệnh lý khác mới vào giai đoạn hoạt hóa Macrophage
5/ Khi nào nghĩ HC thực bào nguyên phát ?
Đáp ứng không tốt với điều trị cơ bản ban đầu
6/Điều trị
Đầu tiên đặt câu hỏi có vào bão Cytokin chưa ?
-Đã có Bão => tập trug xử lý cho ra bão đã => BN chết vì bão
-Chưa có Bão => Từ từ tim nguyên nhân => điều trị tác nhân
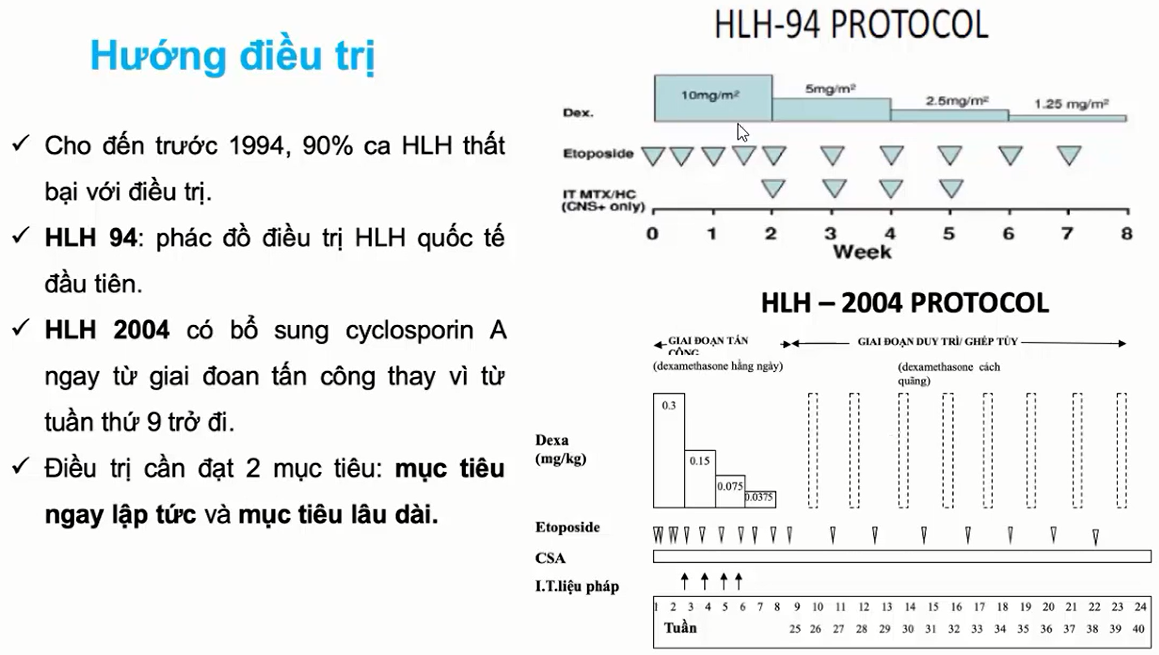
-Điều trị Dexamethasone tấn công 8 tuần
-Sau 8 tuần hết => ngưng
-Sau 8 tuần => có đáp ứng hết sốt nhưng ferritin còn cao, Gan Lách còn to => tiếp tục điều trị duy trì tới mốc 24 tuần hoặc 40 tuần
=> tới mốc 24 tuần nếu tái phát trở lại => Đặt câu hỏi nguyên nhân bẩm sinh có hay không ?
3/ Tại sao không dùng CPT ngay từ đầu mà dùng điện giải rồi mới CPT
-Do cơ thế mất dịch của SXH: dịch thoát khỏi lòng mạch vào khoang thứ 3, vào khoảng kẽ… làm BN tụt huyết áp => sốc
=> Cái mình mong muốn là kéo HA bệnh nhân quay lại sớm từ đầu
-Nếu dùng CPT từ đầu, thì phải truyền lượng dịch rất lớn => nguy cơ phù phổi, RL đông máu…
-Dùng điện giải trước, sẽ bù được ngay lượng dịch để kéo HA trở lại, mặc dù sau đó rất nhanh dịch cũng thoát ra ngoài lòng mạch, thì CPT theo sau sẽ giúp kéo lượng dịch vừa ra ngoài trở lại lòng mạch mà không phải chịu nguy cơ do truyền CPT qua nhiều
4/ Truyền dịch cần chú ý gì
4.1.Đánh giá đáp ứng với LR bằng dấu hiệu gì ?
-Tri giác
-Mạch
-Huyết áp
-CRT
-Nước tiểu
=> Mắc mornitor
-Bơm dịch nếu nhịp tim BN giảm dần, sóng mạch đều => truyền đúng
-Bơm dịch nếu nhịp tim nhanh lên, khám gan to => Xem lại tốc độ truyền hoặc loại sốc xác định đúng chưa
4.2. Đánh giá phù phổi
4.3. Dựa vào sinh hiệu hay hct để giảm dịch ?
=> Sinh hiệu
5. Thể tích tuần hoàn giảm trên 20% => cơ thể mất khả năng bù trừ => suy sụp hệ tuần hoàn
-Khi BN vào sốc, thể tích tuần hoàn đã giảm > 20% => bù dịch lại để phục hồi => kì vọng hct sẽ giảm xuống dưới 20%
-Tuy nhiên, nếu giảm hơn > 20%, ngoài việc pha loãng, cần chú ý thêm tình trạng mất hồng cầu (xuất huyết, có thể xuất huyết vào khoang thứ 3)
Điển hình: đổ 20ml/kg dịch vào mà vẫn không ra sốc + Hct giảm nhanh > 20%
+Nếu kèm huyết động không ổn định nữa => càng ủng hộ có xuất huyết đi kèm ( có thể vào khoang thứ 3 không thấy được)
+ Nếu mạch giảm đều, rõ dần, HA ổn, CRT phục hồi, dịch đã truyền 2-3 liều 20ml/kg Hct mới giảm > 20% => khả năng cao không phải
6. Đường truyền tủy xương
-Dùng trong 6-12 tiếng ( tốt nhất là 6 tiếng => viêm tủy xương)
-Dấu hiệu phải dừng đường truyền tủy xương ngay:
-Phù khớp
-Căng cứng cơ xung quanh, mất mạch ngoại vi phía dưới ( kim đi vào cơ)
-Gãy xương (trẻ nhỏ)
7.Natri máu của BN sốc SXH thường dao động 120-130 mmol/L => Đưa 1 lượng dịch lớn vào cơ thể ( xem nồng độ Natri trong NS và LR) => Giảm Natri do pha loãng
-Tất cả các dịch truyền đều có dung môi pha natri nên việc bù Natri thường không quá cấp thiết (nếu không có dấu hiệu biến chứng)
*Albumin có thể giảm cũng do pha loãng
8. Khám bệnh nhân ban đầu phải đánh giá dấu hiệu suy tim cấp
-Mạch nhanh
-Nhịp tim nhanh, Gallop
-Gan to, Tm cổ nổi, phản hồi Gan – TM Cổ (+)
=> Sau mỗi lần dánh giá đáp ứng, phải đánh giá có dấu hiệu quá tải dịch không
-Suy tim cấp
-Phù phổi cấp: ran phổi, khó thở, trào bọt hồng là đã nặng
9.Khám lâm sàng ban đầu phải chú ý dấu hiệu cảnh báo, yếu tố nguy cơ nặng của BN. Nếu có, lập tức theo dõi tại phòng bệnh nặng hoặc cấp cứu
-Mắc Monitor theo dõi tim , SpO2
-Siêu âm tim, bụng tại giường
=> Không để bệnh nhân đi loạnh quoanh chờ làm XN rồi diễn tiến nặng